Deciphering the Biosimilar vs Generic Drug Differences in Modern Biopharma
The biopharmaceutical industry has entered a transformative era in which the analytical and regulatory principles governing Biosimilar vs Generic Drug Differences have evolved from a reliance on clinical confirmation to an emphasis on advanced structural and functional characterization. While small-molecule generic drugs are exact, chemically synthesized copies of innovator reference products, biosimilars are sophisticated macromolecular biologics produced from living cell lines and must be proven to be highly similar to their reference products.
Need expert support for your regulatory submission? Learn more about our comprehensive biosimilar characterization services.
This fundamental scientific distinction drives markedly different development strategies, clinical requirements, and regulatory approval pathways for each category of drug. As major biologic products approach patent expiration, understanding these technical differences has become increasingly important for regulatory planning and pipeline optimization.
Recent updates from regulatory authorities worldwide have simplified biosimilar development by reducing dependence on extensive human clinical trials and placing greater emphasis on sophisticated in vitro analytical assessments. Biopharmaceutical professionals must understand these evolving standards to effectively manage structural characterization programs, develop robust analytical frameworks, and maintain competitiveness in post-patent markets.
Article Summary:
Article Summary
- Generic drugs are chemically synthesized, low-molecular-weight compounds that are exact copies of reference products, whereas biosimilars are complex biologic medicines produced in living cells and must demonstrate a high degree of similarity to the original biologic.
- Due to their biological origin, biosimilars naturally exhibit minor variations such as glycosylation and other post-translational modifications, making advanced analytical characterization essential for demonstrating comparability.
- Generic drugs are typically approved through the ANDA pathway based on pharmaceutical equivalence and bioequivalence studies, while biosimilars require a comprehensive “totality of evidence” approach that includes analytical, functional, pharmacokinetic, and immunogenicity assessments.
- Regulatory agencies are increasingly prioritizing high-resolution analytical and functional data over extensive comparative clinical efficacy trials, helping reduce biosimilar development costs and timelines.
- Global regulators, including the FDA and EMA, now recognize that approved biosimilars can be considered clinically interchangeable with their reference products in many situations, reducing the need for dedicated switching studies.
- Biosimilar developers rely on risk-based evaluation of Critical Quality Attributes (CQAs) and advanced analytical technologies such as LC-MS/MS, HPLC, capillary electrophoresis, and peptide mapping to establish structural and functional similarity.
- While generic drugs generally require lower investment and reach the market faster, biosimilars involve significantly higher development costs and longer timelines but offer substantial commercial opportunities in the growing biologics market.
Molecular and Manufacturing Dichotomy: Chemical Synthesis vs. Cellular Expression
The identity of a small-molecule generic drug is determined by its precise and reproducible chemical structure, whereas a biosimilar is defined by a large and complex macromolecular structure generated within a living biological system.
Small-molecule drugs, including compounds such as aspirin and certain synthetic peptides, are manufactured through controlled chemical synthesis processes involving sequential reaction steps. This approach enables manufacturers to consistently produce molecules with identical chemical structures from batch to batch.
Because these compounds generally possess low molecular weights, typically below 1,000 Da, and lack intricate higher-order structures, their chemical identity can be confirmed with complete precision at the atomic level.
By comparison, biological therapeutics and biosimilars consist of large, structurally complex, and inherently heterogeneous proteins ranging from approximately 10,000 Da to more than 150,000 Da. These products are manufactured using genetically engineered host systems such as bacterial, yeast, or mammalian cell lines.
Since the production of these macromolecules depends on biological processes occurring within living cells, the resulting drug substance exhibits intrinsic micro-heterogeneity. Even batches manufactured by the original innovator company are not chemically identical to one another.
Ensure your product meets all regulatory standards with our intact mass analysis for biosimilars.
This biological micro-heterogeneity can be illustrated as follows:
Generic Chemical Synthesis
Simple Precursors → Direct Chemical Reactions → Chemically Identical Compound (e.g., Aspirin, 180 Da)
Biological Expression (Biosimilars)
DNA Transfection → Living Host Cell Expression → Complex Folded Macromolecule (e.g., mAb, 150,000 Da)
Inherent variations may include:
- Glycosylation
- Charge variants
- Folding micro-heterogeneity
Living host cells introduce post-translational modifications (PTMs), including N-linked glycosylation, O-linked glycosylation, C-terminal lysine clipping, deamidation, oxidation, and disulfide bond rearrangements. These modifications can influence charge distribution, higher-order structure, and biological activity.
Optimize your characterization strategy by identifying post-translational modifications (PTMs) in biosimilars.
As a result, biosimilar manufacturers must establish highly controlled and reproducible cell lines and culture conditions that closely replicate the target quality attributes of the innovator product. Because the innovator’s original cell line and manufacturing process remain protected as proprietary information, biosimilar developers rely on advanced analytical characterization tools to ensure that any observed micro-heterogeneity remains within clinically acceptable limits.
Navigating Regulatory Pathways and the Core Biosimilar vs Generic Drug Differences
The regulatory framework underlying Biosimilar vs Generic Drug Differences clearly separates simplified bioequivalence-based approvals from the comprehensive analytical and clinical comparability assessments required for biosimilars.
Small-molecule generic drugs are approved through the Abbreviated New Drug Application (ANDA) pathway established under Section 505(j) of the Hatch-Waxman Act. Under this pathway, manufacturers are generally exempt from conducting extensive preclinical safety studies and clinical efficacy trials. Instead, they must demonstrate pharmaceutical equivalence, meaning the product contains the same active ingredient, dosage strength, dosage form, and route of administration as the reference drug, while also establishing bioequivalence.
Bioequivalence is typically demonstrated through pharmacokinetic studies conducted in healthy volunteers. These studies evaluate whether the generic product achieves similar systemic exposure by comparing maximum plasma concentration (Cmax) and area under the concentration-time curve (AUC). Regulatory acceptance generally requires that the 90% confidence interval for the ratio of the generic product to the reference product falls within the established range of 80% to 125%.
Biosimilars, in contrast, are approved through the abbreviated 351(k) Biologics License Application (aBLA) pathway established under the Public Health Service Act (PHSA) and enabled by the Biologics Price Competition and Innovation Act (BPCIA).
Under this framework, a biosimilar may rely on the established safety and efficacy profile of an FDA-licensed 351(a) reference biologic, provided that it can demonstrate a high degree of similarity to the reference product. This requires a comprehensive totality-of-the-evidence package that includes detailed head-to-head structural, functional, pharmacokinetic, and immunogenicity comparisons.
Mitigating Structural Uncertainty and Establishing Biosimilar vs Generic Drug Differences without Clinical Trials
The necessity for comparative clinical efficacy studies (CES) has diminished significantly when analytical similarity between therapeutic proteins can be comprehensively demonstrated.
Historically, biosimilar sponsors were expected to conduct Phase III-style comparative efficacy studies to address any remaining uncertainty regarding clinical performance. However, the FDA’s October 2025 draft guidance, Scientific Considerations in Demonstrating Biosimilarity to a Reference Product: Updated Recommendations for Assessing the Need for Comparative Efficacy Studies, introduced a more streamlined regulatory model.
Drawing on more than a decade of experience evaluating approved biosimilars, the FDA acknowledged that comparative analytical assessments (CAA) are substantially more sensitive than clinical efficacy studies for detecting structural and functional differences between products.
As a result, when high-resolution analytical characterization demonstrates that a biosimilar is highly similar to its reference product, pharmacokinetic similarity studies and immunogenicity assessments are generally sufficient to support regulatory approval. In many cases, extensive comparative clinical efficacy trials are no longer necessary.
This shift has the potential to reduce biosimilar development timelines by one to three years and lower average clinical development costs by as much as 24 million.
Analytical Profiling + PK Similarity + Immunogenicity Assessment ≈ Sufficient for 351(k) BLA Approval
This regulatory evolution is consistent with the 2022 World Health Organization (WHO) Guidelines on the Evaluation of Biosimilars. The WHO encourages National Regulatory Agencies (NRAs) to adopt streamlined approaches that reduce the need for animal toxicity studies and comparative clinical efficacy trials when robust analytical and in vitro functional comparability data are available.
These developments reflect a growing global consensus that detailed physicochemical and functional characterization, rather than clinical endpoint testing, serves as the most reliable foundation for demonstrating therapeutic equivalence in biologic drug development.
Global Alignment and the Shifting Paradigm of Interchangeability
The concept of interchangeability has undergone a significant transformation, moving away from clinical switching studies toward evidence-based analytical determinations.
In the United States, Section 351(k)(4) of the PHSA defines an interchangeable biosimilar as a biological product that satisfies all biosimilarity requirements and may be substituted at the pharmacy level without intervention from the prescribing healthcare provider, similar to traditional generic substitution.
Historically, obtaining this designation required dedicated clinical switching studies. These studies employed crossover designs in which patients alternated between the biosimilar and reference product multiple times to evaluate whether repeated switching affected immunogenicity, safety, or efficacy.
Historical FDA Crossover Trial Design for Interchangeability
Lead-in Period (Reference Product) → Randomized Two-Arm Phase
Arm A: Continuous Reference Product (Non-Switching Control)
Arm B: Multiple Switches (Reference → Biosimilar → Reference → Biosimilar)
To reduce unnecessary clinical burdens and align with international regulatory practices, the FDA released a June 2024 draft guidance entitled Considerations in Demonstrating Interchangeability with a Reference Product: Update.
The updated guidance indicates that clinical switching studies are generally no longer recommended for obtaining interchangeability status. Extensive safety data collected from approved biosimilars demonstrate that switching between biosimilars and reference products does not increase the risk of serious adverse events, immunogenicity, or treatment discontinuation.
This position aligns closely with the European Union’s regulatory framework. In September 2022, the European Medicines Agency (EMA) and the Heads of Medicines Agencies (HMA) jointly stated that any biosimilar approved through the centralized European pathway should be considered clinically interchangeable with its reference product and with other equivalent biosimilars.
After reviewing more than fifteen years of post-marketing safety data, the EMA and HMA concluded that switching between approved biosimilars and reference products does not negatively affect clinical outcomes. Although scientific consensus supports interchangeability across the European Union, decisions regarding automatic pharmacy-level substitution remain the responsibility of individual member states.
Analytical Similarity Assessment and the Tiered Critical Quality Attribute Framework
Analytical similarity assessments require the identification, classification, and statistical evaluation of critical quality attributes (CQAs) that influence the clinical performance of therapeutic proteins.
According to FDA guidance, quality attributes include chemical, physical, biological, and microbiological properties that must remain within established limits to ensure product safety, purity, and efficacy.
Establish a robust foundation for your regulatory filing by defining critical quality attributes (CQAs) in biosimilars.
Biosimilar manufacturers analyze multiple lots of both the biosimilar candidate and the reference product to identify relevant CQAs. These attributes are then categorized according to their potential clinical impact and evaluated using a tiered statistical framework.
Tier 1 (Highest Risk)
Clinical Risk Level: Direct impact on efficacy, safety, potency, or immunogenicity.
Statistical Approach: Rigorous equivalence testing within predefined margins.
Examples: In vitro biological activity assays and receptor-binding affinity measurements such as TNF-alpha binding.
Tier 2 (Moderate Risk)
Clinical Risk Level: Moderate influence on pharmacokinetic or pharmacodynamic properties and safety.
Statistical Approach: Quality range approach using μR ± x·σR.
Examples: N-linked glycan profiles, charge variants, and other post-translational modifications.
Tier 3 (Lowest Risk)
Clinical Risk Level: Minimal impact on clinical outcomes.
Statistical Approach: Descriptive comparisons, visual profiling, and structural fingerprinting.
Examples: Secondary structural elements, general physicochemical properties, structural motifs, and formulation-related attributes.
The statistical rigor applied across these tiers reflects a risk-based approach. For Tier 1 CQAs, analytical similarity is established when the (1−2α)100% two-sided confidence interval for the mean difference between biosimilar and reference lots falls entirely within the predefined similarity margin (−δ, δ).
For Tier 2 CQAs, similarity is demonstrated when a predefined proportion of biosimilar lots, often 90%, falls within a quality range derived from the reference standard deviation and an appropriately justified scaling factor (x).
Tier 3 attributes generally require descriptive comparisons because minor variations in these low-risk attributes are not expected to affect clinical outcomes.
To evaluate these critical attributes comprehensively and eliminate residual uncertainty, developers employ highly sensitive orthogonal analytical methods. Orthogonal approaches use independent technologies based on different physical or chemical principles to assess the same characteristic, minimizing the possibility of analytical blind spots.
Gain deep insights into your protein structure with our glycosylation analysis of biosimilars.
For example, high-performance liquid chromatography (HPLC), including reversed-phase and size-exclusion methodologies, remains the industry standard for purity analysis and aggregate detection at very low levels.
Identify and quantify protein aggregates effectively using aggregation analysis in biosimilars.
These methods are frequently complemented by high-resolution liquid chromatography-mass spectrometry (LC-MS/MS), which confirms molecular mass and identifies sequence modifications with exceptional precision.
Advanced Characterization Technologies
Characterization of monoclonal antibodies and therapeutic peptides requires detailed analysis of charge heterogeneity and post-translational modifications.
Cation-exchange chromatography (CEX) is commonly used to separate and evaluate acidic and basic charge variants. Traditional workflows often require the isolation and subsequent analysis of individual fractions, making the process time-consuming and resource-intensive.
Master complex charge heterogeneity using our charge variant analysis services.
The integration of online native mass spectrometry directly with pH-gradient ion-exchange chromatography has significantly improved efficiency by enabling real-time identification of intact proteoforms and sequence variants.
Additionally, peptide mapping using liquid chromatography-mass spectrometry with alternating low- and high-collision-energy scans (LC-MSE) allows simultaneous confirmation of primary sequence structure, impurity detection, and precise localization of oxidation, deamidation, and disulfide bond arrangements.
Ensure precise primary sequence verification with our peptide mapping in biosimilars.
These advanced orthogonal analytical technologies provide the structural and functional evidence required to support streamlined regulatory submissions and abbreviated clinical development programs.
Economic Realities and Commercialization Strategies in Post-Exclusivity Markets
The economic landscape of post-exclusivity markets reveals substantial differences between generic and biosimilar development models.
Generic drug development follows a relatively low-cost and rapid-entry pathway, typically requiring investments ranging from 1 million to 4 million over approximately three to five years.
Because regulatory requirements are streamlined and manufacturing costs are comparatively low, numerous generic competitors often enter the market immediately after patent expiration. This competition frequently drives prices down by 80% to 90% relative to the branded product.
Biosimilar development, however, represents a long-term and capital-intensive investment strategy. Development programs often require expenditures exceeding 100 million and may take eight to ten years to reach commercialization.
The complexity of mammalian cell line engineering, bioreactor process optimization, and comparative analytical and pharmacological assessments contributes significantly to these higher costs.
Given the substantial infrastructure requirements and stringent quality standards associated with biologic manufacturing, market entry barriers remain high. Consequently, biosimilar markets generally experience more gradual price reductions, with discounts typically ranging from 15% to 35% compared with reference biologics.
This pricing model supports sustainable long-term profitability despite a smaller number of market participants.
Development and Commercial Parameters
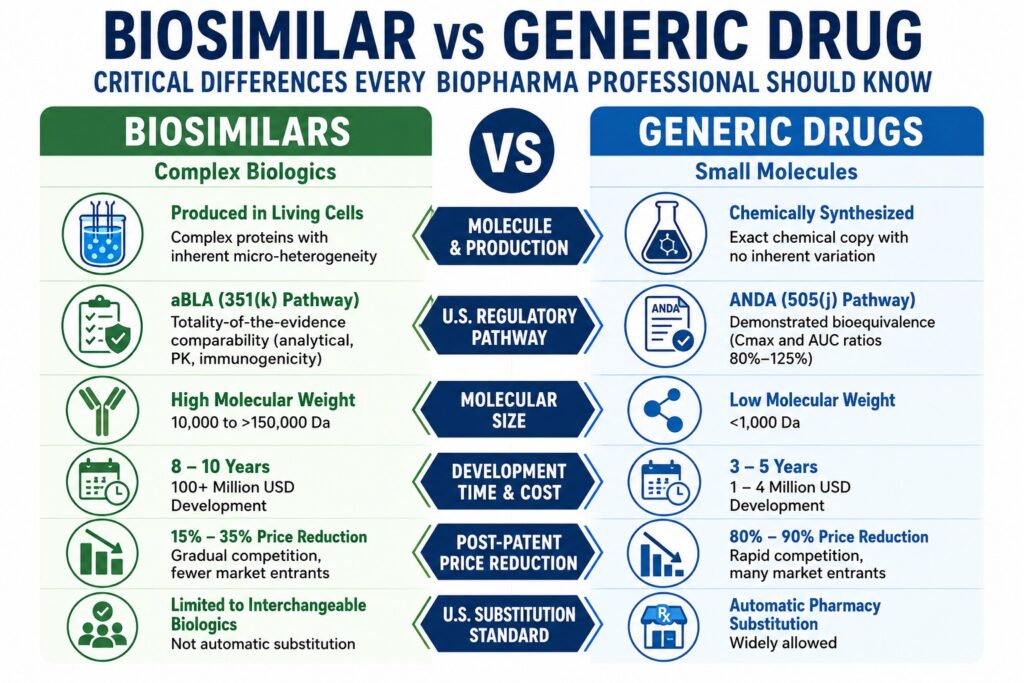
Typical Molecular Weight
- Generic Drugs: Low molecular weight (<1,000 Da)
- Biosimilars: High molecular weight (10,000 to >150,000 Da)
Active Ingredient
- Generic Drugs: Exact chemical copy
- Biosimilars: Highly similar with expected biological variation
U.S. Regulatory Filing
- Generic Drugs: ANDA
- Biosimilars: aBLA
Statutory Pathway
- Generic Drugs: Section 505(j) of the FD&C Act
- Biosimilars: Section 351(k) of the PHS Act
Primary Approval Requirement
- Generic Drugs: Demonstrated bioequivalence (Cmax and AUC ratios)
- Biosimilars: Head-to-head totality-of-the-evidence similarity
Average Development Budget
- Generic Drugs: 1 million to 4 million
- Biosimilars: 100 million or more
Average Development Timeline
- Generic Drugs: 3 to 5 years
- Biosimilars: 8 to 10 years
Post-Patent Price Reduction
- Generic Drugs: 80% to 90%
- Biosimilars: 15% to 35%
U.S. Substitution Standard
- Generic Drugs: Automatic pharmacy substitution
- Biosimilars: Limited to interchangeable biologics
Strategic Integration: Supporting Regulatory Filings with Analytical Precision
Comprehensive analytical characterization generated by qualified scientific partners forms the foundation of successful generic and biosimilar regulatory submissions.
As regulatory authorities increasingly require high-resolution analytical evidence to establish product sameness or similarity, selecting the right analytical partner has become a strategic component of drug development.
To support these demanding development programs, ResolveMass Laboratories Inc. provides specialized analytical services designed for both generic and biosimilar manufacturers.
Operating as a USFDA-registered facility with FDA Establishment Identifier (FEI: 3042696771) and an ISO 9001:2015-certified Quality Management System, the laboratory delivers regulatory-ready analytical data that meets global compliance standards.
ResolveMass Laboratories Inc. combines advanced instrumentation with a team of PhD-level scientists to assist developers in confirming product sameness, characterizing impurities, and defining macromolecular structures.
The laboratory’s core technical capabilities include:
Peptide API Characterization
Peptide sequencing, impurity profiling using LC-MS/MS, and high-performance liquid chromatography (HPLC-UV with C18 columns at 214 nm and 280 nm) to support ANDA sameness requirements.
Advanced Macromolecular Analysis
High-resolution Orbitrap mass spectrometry, quantitative nuclear magnetic resonance (qNMR), capillary electrophoresis (CE), and MALDI-TOF mass spectrometry for higher-order structural characterization and sequence verification.
Biodegradable Polymer Synthesis
Custom synthesis and molecular-weight determination using GPC for PLGA, PLA, and PLCL polymers intended for long-acting injectable drug delivery systems.
Impurity and Impurity Profiling
Sensitive analytical testing for nitrosamines, PFAS contamination in drug matrices, and extractables and leachables (E&L) assessments to support product safety and regulatory compliance.
Conclusion
A thorough understanding of the molecular, analytical, and regulatory Biosimilar vs Generic Drug Differences is critical for biopharmaceutical organizations seeking success in post-patent markets while minimizing development risk.
Although small-molecule generic drug development remains a proven and efficient business model, biosimilars represent a high-value growth opportunity supported by evolving regulatory frameworks that increasingly prioritize analytical comparability over extensive clinical testing.
Collaborating with an experienced analytical contract research organization (CRO) helps ensure that characterization packages satisfy the rigorous expectations of global regulatory authorities.
Get the data you need for successful comparability studies. Explore our biosimilar comparability studies.
To discuss analytical characterization requirements, custom polymer synthesis projects, or advanced impurity profiling services with the scientific team, please visit the ResolveMass Contact Page.
Frequently Asked Questions
Biosimilars are not considered generic biologics because biologic medicines are produced using living cells, making exact replication impossible. Natural biological processes can introduce minor variations, including differences in glycosylation patterns, charge distribution, and other post-translational modifications. Unlike generic drugs, which are chemically identical copies, biosimilars are developed to be highly similar to the reference biologic without causing any clinically meaningful differences in safety, efficacy, or quality.
The financial and operational requirements for biosimilars are significantly greater than those for generic drugs. A generic product can often be developed within 3 to 5 years at a cost of approximately 1 million to 4 million. In contrast, biosimilar development commonly requires investments exceeding 100 million and may take 8 to 10 years due to extensive analytical characterization, cell line development, manufacturing optimization, and clinical pharmacology evaluations.
To obtain regulatory approval, a generic drug must demonstrate bioequivalence to its reference product. This means the active ingredient must reach the bloodstream at a comparable rate and extent. Pharmacokinetic studies evaluate parameters such as maximum plasma concentration (Cmax) and area under the curve (AUC). Regulatory agencies generally require the 90% confidence intervals for these measurements to fall within the accepted range of 80% to 125% relative to the reference product.
Orthogonal testing improves confidence in analytical results by using multiple independent techniques to evaluate the same critical quality attribute. Since each analytical method measures properties differently, combining approaches helps identify variations that could otherwise go undetected. For example, using both reversed-phase HPLC and capillary electrophoresis provides complementary information about purity and molecular characteristics, helping ensure a thorough assessment of biosimilarity.
The European Union takes a broader scientific approach to interchangeability. Regulatory authorities such as the EMA and HMA have stated that approved biosimilars can generally be considered interchangeable with their reference products. Historically, the USFDA maintained a separate designation requiring additional evidence before pharmacy-level substitution was allowed. However, recent regulatory updates in the United States have moved toward greater alignment with the European model by reducing the need for extensive switching studies.
Critical Quality Attributes (CQAs) are measurable physical, chemical, biological, or microbiological characteristics that directly influence the quality and performance of a therapeutic product. For biosimilar evaluations, these attributes are grouped into three risk-based tiers. Tier 1 includes attributes with the greatest impact on safety and efficacy, Tier 2 covers characteristics with moderate clinical relevance, and Tier 3 includes low-risk properties that are typically assessed through descriptive comparisons.
Mass spectrometry and peptide mapping are powerful analytical tools used to verify the molecular structure of biosimilars. These techniques enable scientists to confirm amino acid sequences, detect impurities, and identify post-translational modifications such as oxidation, deamidation, and glycosylation changes. By providing detailed structural information, they help establish biosimilarity and generate the robust analytical evidence required for regulatory submissions.
Reference:
- U.S. Food and Drug Administration. (2025, October 29). Scientific considerations in demonstrating biosimilarity to a reference product: Updated recommendations for assessing the need for comparative efficacy studies: Draft guidance for industry. U.S. Department of Health and Human Services. https://www.fda.gov/media/189366/download
- U.S. Food and Drug Administration. (2025, October 29). FDA moves to accelerate biosimilar development and lower drug costs. U.S. Department of Health and Human Services. https://www.fda.gov/news-events/press-announcements/fda-moves-accelerate-biosimilar-development-and-lower-drug-costs
- U.S. Food and Drug Administration. (n.d.). 9 things to know about biosimilars and interchangeable biosimilars. U.S. Department of Health and Human Services. https://www.fda.gov/drugs/things-know-about/9-things-know-about-biosimilars-and-interchangeable-biosimilars
- Liu, Y., Lou, W., & Chow, S.-C. (2026). Switching design for assessment of interchangeability in biosimilar studies. Pharmaceutics, 18(2), 187. https://doi.org/10.3390/pharmaceutics18020187
- U.S. Food and Drug Administration. (2024, June). Considerations in demonstrating interchangeability with a reference product: Update: Draft guidance for industry. U.S. Department of Health and Human Services. https://www.fda.gov/media/179456/download
- Chow, S.-C., Song, F., & Bai, H. (2016). Analytical similarity assessment in biosimilar studies. The AAPS Journal, 18(3), 670–677. https://doi.org/10.1208/s12248-016-9882-5
- Hong, J., Lee, Y., Li, N., Yang, J., Han, J., Lee, H. J., Lee, S. C., Song, K. W., & Tsai, N. (2011). Rapid comparison of a candidate biosimilar to an innovator monoclonal antibody with advanced liquid chromatography and mass spectrometry technologies. mAbs, 3(5), 466–477. https://doi.org/10.4161/mabs.3.5.17008

