Introduction: The Bioanalytical Complexity of ADC Programs
Bioanalysis for an Antibody-Drug Conjugate Program is far from a straightforward analytical exercise. It represents one of the most technically challenging areas in modern drug development because it requires the simultaneous evaluation of chemically and structurally distinct analytes within the same biological matrix. Unlike traditional small molecule or biologic development programs that generally depend on a single primary assay, ADC programs inherently require at least three separate analytical viewpoints: total antibody (TAb), conjugated payload, and free (unconjugated) payload. Each analyte possesses unique molecular characteristics, including different molecular weights, polarity profiles, stability behaviors, and plasma concentration ranges, making simultaneous quantitation highly complex from a bioanalytical standpoint.
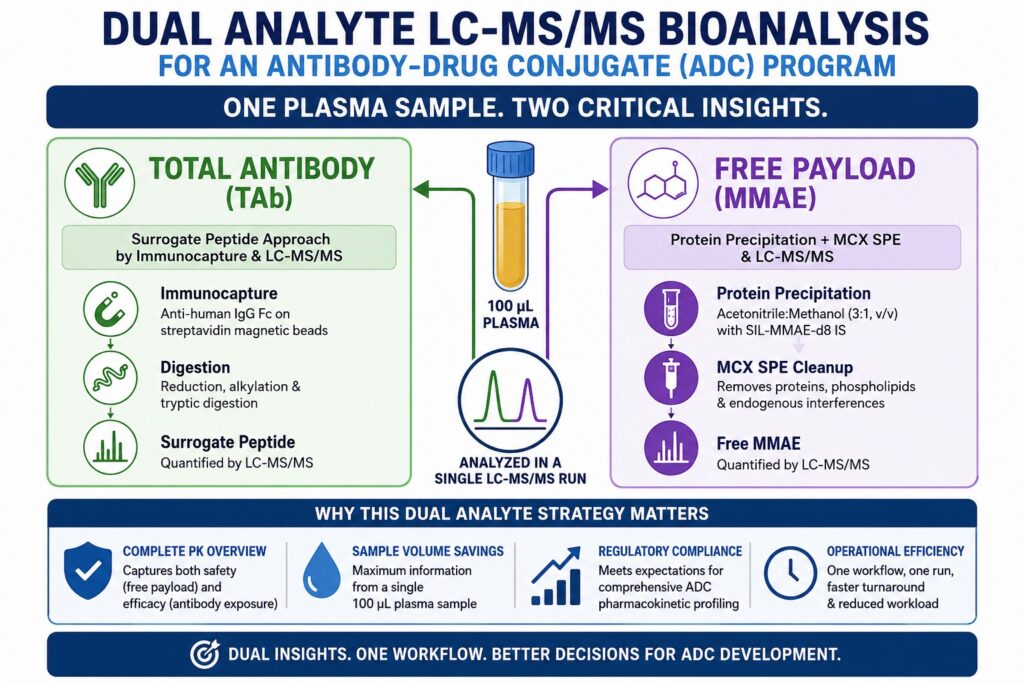
This case study outlines the complete development, validation, and clinical application of a dual analyte LC-MS/MS assay capable of simultaneously quantifying free small-molecule payload and total antibody through a surrogate peptide approach. The assay was developed for a clinical-stage ADC program targeting a solid tumor indication. The ADC consisted of an IgG1 monoclonal antibody conjugated to monomethyl auristatin E (MMAE) through a protease-cleavable linker, with a nominal drug-to-antibody ratio (DAR) of 4.
The decision to combine both analytes into a unified analytical platform was driven by three primary considerations:
- Regulatory expectations requiring comprehensive pharmacokinetic characterization at every study time point
- Sample volume limitations in early clinical cohorts, necessitating maximum analytical information from minimal plasma volume
- Accelerated development timelines, where maintaining two fully validated standalone methods would substantially increase analytical workload and reporting turnaround times
Discover how specialized expertise can streamline your development timeline: Learn more about our Outsourced Bioanalytical Services.
Share via:
Article Summary:
- Dual analyte LC-MS/MS enables concurrent measurement of free payload and total antibody using a single plasma aliquot, significantly improving efficiency and reducing reporting timelines in ADC pharmacokinetic (PK) investigations.
- This case study outlines the scientific basis for analyte selection, integrated sample preparation using immunocapture and enzymatic digestion, key method development considerations, regulatory validation requirements, and clinical pharmacokinetic findings generated during the study.
- One of the primary bioanalytical complexities in ADC development is that free payload and total antibody circulate at substantially different concentration levels in plasma, making it necessary to apply separate extraction approaches within one coordinated analytical workflow.
- The fully validated dual analyte LC-MS/MS assay demonstrated a lower limit of quantification (LLOQ) of 1.0 ng/mL for free payload and 0.50 µg/mL for the total antibody surrogate peptide in human plasma while remaining compliant with established regulatory acceptance criteria.
- Method validation was conducted according to FDA Bioanalytical Method Validation Guidance (2018) and ICH M10 recommendations, including comprehensive assessment of accuracy, precision, selectivity, matrix effects, dilution integrity, and analyte stability.
- Simultaneous monitoring of both analytes also supports estimation of temporal Drug-to-Antibody Ratio (DAR) changes, providing valuable insight into ADC pharmacokinetic and pharmacodynamic behavior.
- The use of stable isotope-labeled (SIL) internal standards for both payload and surrogate peptide analysis played a critical role in minimizing matrix-related ion suppression and reducing inter-run analytical variability.
Defining the Dual Analyte Strategy: Why These Two Analytes?
The two selected analytes, free payload and total antibody, were chosen because together they provide the most clinically meaningful and safety-relevant pharmacokinetic overview of ADC behavior in systemic circulation.
In this development program, the ADC carried MMAE as the cytotoxic payload attached through a valine-citrulline (vc) protease-cleavable linker. During systemic circulation, two major biological processes influence the therapeutic balance between efficacy and toxicity:
Premature Payload Release
Free MMAE present in systemic circulation is the primary contributor to off-target toxicities such as peripheral neuropathy and neutropenia. Measuring free MMAE concentrations at each pharmacokinetic time point is essential for establishing exposure-toxicity relationships and understanding systemic safety risk.
Antibody Deconjugation and Clearance
Total antibody concentration, including both conjugated and unconjugated antibody forms, reflects the overall persistence and half-life of the therapeutic antibody component. This parameter directly informs dosing interval selection and overall pharmacokinetic behavior.
Monitoring only one analyte would generate an incomplete and potentially misleading pharmacokinetic interpretation. For example, a reduction in total antibody exposure without a corresponding increase in free payload concentrations may indicate acceptable linker stability. In contrast, divergence between the two concentration-time profiles can indicate accelerated deconjugation, which represents a significant safety concern.
Align your drug development program with international standards: Explore our Biomarker Bioanalytical Services for FDA and Health Canada.
Why Not Include Three or Four Analytes?
A fully comprehensive ADC bioanalytical strategy may include additional analytes such as conjugated antibody, naked antibody (DAR = 0), average DAR, and total payload. However, for early clinical pharmacokinetic support in this program, the dual analyte strategy consisting of free payload and total antibody was considered the optimal balance between regulatory expectations, analytical complexity, and operational feasibility.
| Analyte Combination | Regulatory Requirement | Analytical Complexity | Program Stage Fit |
|---|---|---|---|
| Free Payload only | Minimum safety requirement | Low | Discovery |
| Free Payload + TAb | Recommended for IND/CTA support | Moderate | Phase I/II ✓ |
| Free Payload + TAb + Conjugated Ab | Comprehensive PK characterization | High | Phase II/III |
| Full DAR-resolved panel | Complete mechanistic understanding | Very High | Late-phase |
Secure a reliable partner for early-phase clinical testing: Learn more about our Biomarker Bioanalytical Services CRO.
Sample Preparation Architecture: A Split-Path Workflow in a Single Tube
The central innovation of this dual analyte assay was the implementation of a bifurcated extraction workflow that processed a single 100 µL plasma aliquot through two independent preparation pathways before final LC-MS/MS analysis.
This represented the most technically challenging stage of assay development because the two analytes required fundamentally incompatible extraction conditions.
Free MMAE Extraction Requirements
Free MMAE, with a molecular weight of approximately 718 Da, required organic protein precipitation using acetonitrile/methanol (3:1, v/v), followed by mixed-mode cation exchange (MCX) solid-phase extraction to enrich the analyte and remove endogenous phospholipids and plasma contaminants.
Total Antibody Surrogate Peptide Preparation
The surrogate peptide generated from tryptic digestion of the antibody complementarity-determining region (CDR) required a completely different preparation workflow. This included immunocapture using a biotinylated anti-human IgG Fc antibody immobilized on streptavidin magnetic beads, followed by denaturation, reduction, alkylation, and enzymatic digestion to release the unique surrogate peptide sequence EIVLTQSPATLSLSPGER.
Accelerate your early-stage pipeline with robust assay design: Explore our Bioanalytical CRO for Drug Discovery.
Sample Preparation Workflow
Plasma Sample (100 µL)
Part A: Total Antibody Analysis (60 µL)
- Addition of biotinylated anti-human IgG Fc capture antibody
- Incubation with streptavidin magnetic beads for 1 hour at room temperature
- Triple wash using PBS-T buffer
- Elution followed by reduction using DTT at 56°C for 30 minutes and alkylation using iodoacetamide
- Overnight trypsin digestion at 37°C for 18 hours
- Addition of stable isotope-labeled (SIL) surrogate peptide internal standard and quenching with formic acid
- Injection volume: 10 µL
Part B: Free MMAE Analysis (40 µL)
- Addition of SIL-MMAE-d8 internal standard
- Protein precipitation using acetonitrile:methanol (3:1, v/v) at four times the plasma volume
- Centrifugation at 3000 rpm for 10 minutes at 4°C
- Loading of supernatant onto MCX SPE cartridge
- Sequential washing using water followed by 5% methanol
- Elution using 5% ammonium hydroxide in methanol
- Evaporation to dryness and reconstitution in 50 µL of 0.1% formic acid in water
- Injection volume: 5 µL
Both prepared extracts were analyzed within the same LC-MS/MS run sequence using a column-switching valve system that directed each analyte-specific extract to its designated chromatographic column.
Chromatographic Conditions
Free MMAE
- Column: Kinetex C18 (2.6 µm, 50 × 2.1 mm)
- Mobile phase: 0.1% formic acid in water/acetonitrile gradient
Surrogate Peptide
- Column: Acquity UPLC BEH C18 (1.7 µm, 100 × 2.1 mm)
- Mobile phase: 0.1% formic acid in water/acetonitrile gradient
Mass Spectrometry Parameters and Selectivity
MRM transitions for both analytes were carefully optimized to maximize selectivity against endogenous plasma components and ADC-related catabolites.
Detection was performed using an AB SCIEX 7500 triple-quadrupole mass spectrometer operated in positive electrospray ionization (ESI) mode.
MRM Transitions
| Analyte | Precursor Ion (m/z) | Product Ion (m/z) | Collision Energy (eV) | DP (V) |
|---|---|---|---|---|
| Free MMAE | 718.5 [M+H]⁺ | 152.1 | 35 | 100 |
| Free MMAE (qualifier) | 718.5 | 686.5 | 22 | 100 |
| MMAE-d8 IS | 726.5 [M+H]⁺ | 152.1 | 35 | 100 |
| Surrogate Peptide | 682.9 [M+2H]²⁺ | 947.5 (y8) | 28 | 80 |
| SIL Surrogate Peptide IS | 688.9 [M+2H]²⁺ | 959.5 (y8*) | 28 | 80 |
The use of a secondary qualifier transition for free MMAE was particularly important for confirming chromatographic peak identity and eliminating the possibility of interference from structurally related catabolites such as MMAF and des-methyl MMAE.
Optimize characterization for your safety and efficacy trials: Check out our Bioanalytical CRO Services for PK and TK.
Method Validation: Key Outcomes Against FDA/ICH M10 Criteria
Complete method validation was performed in accordance with the FDA Bioanalytical Method Validation Guidance (2018) and ICH M10 (2022). Both analytes were validated in human K₂EDTA plasma using six independent lots obtained from drug-naïve donors.
Calibration Range and LLOQ
| Analyte | LLOQ | ULOQ | Calibration Model |
|---|---|---|---|
| Free MMAE | 1.0 ng/mL | 500 ng/mL | Weighted 1/x² linear |
| Total Antibody Surrogate Peptide | 0.50 µg/mL | 200 µg/mL | Weighted 1/x² linear |
Both analytes demonstrated correlation coefficients (r²) greater than 0.999 across five independent calibration curves.
Accuracy and Precision
| Parameter | Free MMAE (% CV) | Free MMAE (% Bias) | Surrogate Peptide (% CV) | Surrogate Peptide (% Bias) |
|---|---|---|---|---|
| Intra-run precision | ≤8.2% | ±4.6% | ≤7.9% | ±5.1% |
| Inter-run precision | ≤11.4% | ±7.8% | ≤10.7% | ±6.3% |
| LLOQ precision | ≤18.6% | ±14.2% | ≤17.9% | ±13.8% |
All validation parameters satisfied FDA and ICH M10 acceptance criteria of ≤15% variability, or ≤20% at the LLOQ level.
Matrix Effect Assessment
Matrix suppression represented a major concern because of the dual analyte assay design. Post-column infusion experiments and IS-normalized matrix factor evaluations were conducted.
- Free MMAE IS-normalized matrix factor: 0.94–1.07 across six plasma lots
- Surrogate peptide IS-normalized matrix factor: 0.89–1.11 across six plasma lots
No unacceptable matrix effects were observed in hemolyzed or lipemic samples, confirming the effectiveness of both the MCX SPE cleanup procedure and the immunocapture workflow.
Stability Assessment
| Stability Condition | Free MMAE | Surrogate Peptide |
|---|---|---|
| Bench-top (6 hr, RT) | Stable (≤5.2% deviation) | Stable (≤4.8% deviation) |
| Freeze-thaw (5 cycles) | Stable (≤8.4% deviation) | Stable (≤7.6% deviation) |
| Long-term frozen (−70°C, 90 days) | Stable (≤10.1% deviation) | Stable (≤9.3% deviation) |
| In-injector (24 hr, 5°C) | Stable (≤7.7% deviation) | Stable (≤6.9% deviation) |
| Processed sample (24 hr, 5°C) | Stable (≤9.2% deviation) | Stable (≤8.1% deviation) |
| Whole blood (2 hr, RT) | Stable (≤11.8% deviation) | Not applicable |
The whole blood stability study was especially important because it confirmed that clinical samples processed within the predefined 2-hour collection-to-centrifugation window would not produce artificially elevated free payload concentrations due to ex vivo linker cleavage or adsorption to cellular blood components.
Leverage state-of-the-art gold standard instrumentation: Learn more about our LC-MS/MS Bioanalytical Services.
Application to the Phase I Clinical PK Study
The validated dual analyte assay was subsequently applied to 847 clinical samples collected from 38 patients enrolled in a first-in-human dose escalation study involving three dose cohorts: 1.2, 1.8, and 2.4 mg/kg IV administered every three weeks (Q3W). This generated the first simultaneous pharmacokinetic profiles for both free payload and total antibody in human subjects for this ADC.
Key Pharmacokinetic Findings
- Total antibody demonstrated a characteristic biphasic pharmacokinetic profile with a mean terminal half-life of approximately 7–9 days. This was consistent with expected IgG1 clearance behavior and slightly faster than the unconjugated parent monoclonal antibody, reflecting conjugation-associated alterations in FcRn recycling.
- Free MMAE concentrations remained detectable above the LLOQ at all time points within the first 72 hours after infusion. Peak plasma concentrations (Cmax) occurred approximately 2–4 hours post-dose, confirming rapid initial payload release during the early distribution phase.
- The ratio of total antibody exposure to free payload exposure increased proportionally with dose escalation. This suggested saturation of target-mediated drug disposition (TMDD) pathways at higher dose levels, resulting in non-linear pharmacokinetics and providing critical information for Phase II dose selection.
Surrogate DAR Calculation from Dual Analyte Data
One of the most valuable analytical advantages of the dual analyte platform was the ability to estimate circulating average DAR values over time using the molar relationship between conjugated payload and total antibody concentrations. Although this represented a surrogate DAR estimate rather than a true DAR-resolved LC-MS characterization, it provided highly informative real-time insight into linker stability in vivo.
Surrogate DAR(t)=[Conjugated Payload concentration (μmol/L)][Total Antibody concentration (μmol/L)]\mathrm{Surrogate\ DAR}(t)=\frac{[\mathrm{Conjugated\ Payload\ concentration}\ (\mu mol/L)]}{[\mathrm{Total\ Antibody\ concentration}\ (\mu mol/L)]}Surrogate DAR(t)=[Total Antibody concentration (μmol/L)][Conjugated Payload concentration (μmol/L)]
Within this program, the surrogate DAR decreased from approximately 3.8 at Cmax to approximately 1.9 by Day 14, indicating moderate in vivo deconjugation characteristic of vc-MMAE linker systems. While this did not represent a direct safety concern, it provided an important pharmacokinetic and pharmacodynamic modeling parameter.
Transition smoothly from assay design to regulatory success: Explore our Bioanalytical Method Development and Validation.
Analytical Challenges Encountered and Solutions Applied
Challenge 1: Cross-Contamination of Free Payload Signal During Protein Precipitation
When protein precipitation was performed on plasma samples containing high ADC concentrations (>100 µg/mL total antibody), artificially elevated free MMAE concentrations were observed due to partial hydrolysis of the vc linker in acidic acetonitrile conditions.
Solution
The MCX SPE conditioning protocol was modified to include a 1 mL wash using 0.5% formic acid in water before analyte elution. This effectively removed low-molecular-weight linker fragments while retaining intact MMAE. In addition, the protein precipitation temperature was reduced to −20°C rather than room temperature to minimize ex vivo linker cleavage.
Challenge 2: Variability in Trypsin Digest Efficiency
Incomplete tryptic digestion of the antibody heavy chain initially resulted in inter-run variability exceeding 22% CV, surpassing ICH M10 acceptance criteria.
Solution
A dual-enzyme digestion strategy was introduced using a 2-hour Lys-C pre-digestion step followed by trypsin digestion. This increased digestion completeness to greater than 95% and reduced inter-run variability to below 11% CV across all QC levels.
Challenge 3: Phospholipid Interference at the MMAE LLOQ
Phospholipid species, particularly phosphatidylcholine (PC) and lysophosphatidylcholine (LPC), produced ion suppression affecting the MMAE MRM transition in hemolyzed plasma samples.
Solution
An additional phospholipid removal step using Ostro Pass-Through sample preparation plates was introduced after protein precipitation and before MCX SPE loading. This reduced phospholipid signal intensity by approximately 94% and eliminated matrix suppression at the LLOQ level.
Maximize asset value even with lean virtual operations: Check out our specialized Bioanalytical CRO for Virtual Biotech.
Regulatory Submission and GLP Compliance Considerations
The dual analyte method was executed under full GLP conditions in support of the Phase I IND submission. Major regulatory documentation components included:
- Independent validation reports for each analyte, despite operation on a shared analytical platform, in accordance with FDA recommendations for assays involving different calibration ranges
- Selectivity assessments against commonly co-administered medications including paclitaxel, carboplatin, and dexamethasone to confirm the absence of clinically relevant analytical interference
- Cross-validation against a previously validated ELISA-based total antibody assay using a 10% incurred sample subset to establish cross-platform comparability
- Stability bridging studies comparing clinical site freezer storage conditions (−20°C) versus central laboratory storage conditions (−70°C), confirming no statistically significant concentration differences for up to 14 days at −20°C
Maintain rigid verification for every study milestone: Review our guidelines on Bioanalytical Data Integrity.
Strategic Takeaways for ADC Bioanalytical Program Design
Based on the experience from this case study, several strategic principles emerged that are broadly applicable to bioanalysis for an Antibody-Drug Conjugate Program.
Define Analyte Prioritization Early
The decision to pursue a dual analyte or expanded multi-analyte strategy should be established at program initiation rather than retrospectively. The selection must align with program stage, regulatory expectations, and sample volume limitations.
Prioritize Internal Standard Strategy
Stable isotope-labeled peptides for antibody surrogate quantitation and deuterium-labeled payload standards are essential for achieving GLP-grade analytical precision. Commercial availability of SIL standards for common payloads such as MMAE, DXd, SN-38, and MMAF continues to improve.
Address Linker Lability During Method Development
Ex vivo linker cleavage artifacts should be identified and controlled during development using spiked ADC samples at clinically relevant concentrations. Linker instability remains one of the most common causes of validation failure in ADC bioanalysis.
Utilize Simultaneous DAR Monitoring
When both free payload and total antibody are already being quantified, surrogate DAR calculations can be generated without additional assay development investment, significantly enhancing pharmacokinetic and pharmacodynamic interpretation.
Establish Parallelism Early
Dilution series evaluations using incurred clinical samples should be performed early in development to confirm consistent immunocapture efficiency across all clinically relevant concentration ranges.
Navigate the complexities of cutting-edge biotherapeutics: Read about our Antibody-Drug Conjugate Bioanalytical Services.
Conclusion: Advancing Bioanalysis for an Antibody-Drug Conjugate Program
This case study demonstrates that a carefully optimized and fully validated dual analyte LC-MS/MS assay is not only technically achievable, but also represents an analytically and operationally superior strategy for supporting Phase I pharmacokinetic studies in ADC development programs. By integrating free payload quantitation through small-molecule SPE-LC-MS/MS with total antibody analysis through immunocapture peptide-LC-MS/MS into a unified workflow, the program achieved complete regulatory compliance, significant conservation of clinical sample volume, and simultaneous pharmacokinetic characterization capable of supporting surrogate DAR trending, all from a single 100 µL plasma aliquot collected at each time point.
For development teams advancing bioanalysis for an Antibody-Drug Conjugate Program through regulatory submissions, the dual analyte LC-MS/MS strategy represents the current state-of-the-art approach for Phase I pharmacokinetic support. The methodology described in this case study satisfied all FDA Bioanalytical Method Validation and ICH M10 acceptance criteria and successfully generated pharmacokinetic data that directly informed dose selection decisions for subsequent Phase II clinical development.
Frequently Asked Questions (FAQs)
In ADC bioanalysis, free payload refers to the cytotoxic drug that has separated from the antibody and is circulating independently in the bloodstream. This free drug is closely associated with systemic toxicity and adverse effects because it can interact with healthy tissues outside the target site. Total antibody, on the other hand, measures the entire monoclonal antibody component regardless of whether the payload remains attached. Evaluating both analytes together provides a complete understanding of ADC pharmacokinetics, linker stability, therapeutic exposure, and overall safety behavior.
LC-MS/MS is widely preferred for ADC payload analysis because it offers highly specific molecular detection based on mass-to-charge ratios and selective MRM transitions. Unlike ELISA, which may suffer from cross-reactivity, limited dynamic range, or hook effects, LC-MS/MS can accurately detect very low payload concentrations even in complex plasma matrices. The combination of SPE cleanup and tandem mass spectrometry also improves sensitivity for sub-nanogram-level quantification. This makes LC-MS/MS particularly valuable when high circulating ADC concentrations could interfere with antibody-based assays.
Immunocapture is a selective extraction technique used to isolate the antibody portion of an ADC from biological samples before LC-MS/MS analysis. In this process, a biotinylated anti-human IgG antibody is attached to streptavidin-coated magnetic beads, allowing selective binding of the ADC antibody from plasma. After several wash steps remove unwanted matrix components, the captured antibody undergoes enzymatic digestion using trypsin or a multi-enzyme digestion strategy. This releases a unique surrogate peptide from the CDR region, which is then quantified as a representative marker of total antibody concentration.
Drug-to-Antibody Ratio, commonly abbreviated as DAR, represents the average number of payload molecules attached to each monoclonal antibody. DAR is one of the most important parameters influencing ADC potency, pharmacokinetics, and stability. In plasma studies, DAR is commonly estimated using the molar ratio between payload concentration and total antibody concentration obtained through LC-MS/MS analysis. More advanced characterization methods, such as intact protein mass spectrometry or high-resolution mass spectrometry, can provide DAR species distribution, although these techniques are generally reserved for specialized characterization studies rather than routine clinical PK analysis.
ICH M10 and FDA Bioanalytical Method Validation guidance establish strict criteria for validating ADC bioanalytical methods to ensure reliability and regulatory compliance. Both guidelines require evaluation of assay accuracy, precision, selectivity, matrix effects, dilution integrity, and analyte stability under all relevant storage and processing conditions. Acceptance limits generally require accuracy within ±15% of nominal values and precision below 15% CV, except at the LLOQ where ±20% is acceptable. For ADC-specific methods, additional focus is placed on linker stability, carry-over risk, and potential interference from conjugated or deconjugated species within the sample matrix.
Preventing ex vivo payload release is essential for maintaining accurate ADC pharmacokinetic data during sample handling and preparation. Temperature control plays the most critical role, and samples are typically maintained at 4°C or lower immediately after collection. Cold organic precipitation conditions, such as protein precipitation at −20°C, help suppress unwanted chemical or enzymatic linker cleavage. Rapid plasma separation, minimized processing delays, and the use of protease inhibitor cocktails further reduce the likelihood of artificial payload release. Additional SPE cleanup steps can also remove linker-related fragments before LC-MS/MS analysis.
Stable isotope-labeled internal standards are considered the preferred option for dual analyte ADC assays because they provide the highest level of analytical accuracy and reproducibility. For payload quantification, deuterated or isotopically labeled versions of the payload, such as MMAE-d8 or DXd-d5, are commonly used. For antibody surrogate peptide analysis, fully labeled ¹³C/¹⁵N peptide standards are recommended to compensate for variability during immunocapture and enzymatic digestion. Although structurally similar analog standards may sometimes be used, they generally provide lower correction efficiency and may face greater scrutiny during regulatory review.
Linker chemistry has a major influence on ADC bioanalysis because it determines payload release behavior, analyte selection, and sample preparation requirements. Cleavable linkers, such as valine-citrulline or disulfide linkers, can release free payload in circulation, making free payload monitoring especially important for evaluating toxicity risk. Non-cleavable linkers behave differently because they generate amino acid-payload catabolites instead of releasing intact payload molecules. As a result, different analytical standards, extraction procedures, and MRM transitions may be required depending on linker type. Cleavable linker ADCs also demand stricter cold-chain handling to minimize ex vivo degradation artifacts.
Reference:
- US FDA. Bioanalytical Method Validation Guidance for Industry. 2018. https://www.fda.gov/media/70858/download
- ICH. M10 Bioanalytical Method Validation and Study Sample Analysis. 2022. https://www.ich.org/page/multidisciplinary-guidelines

