Introduction
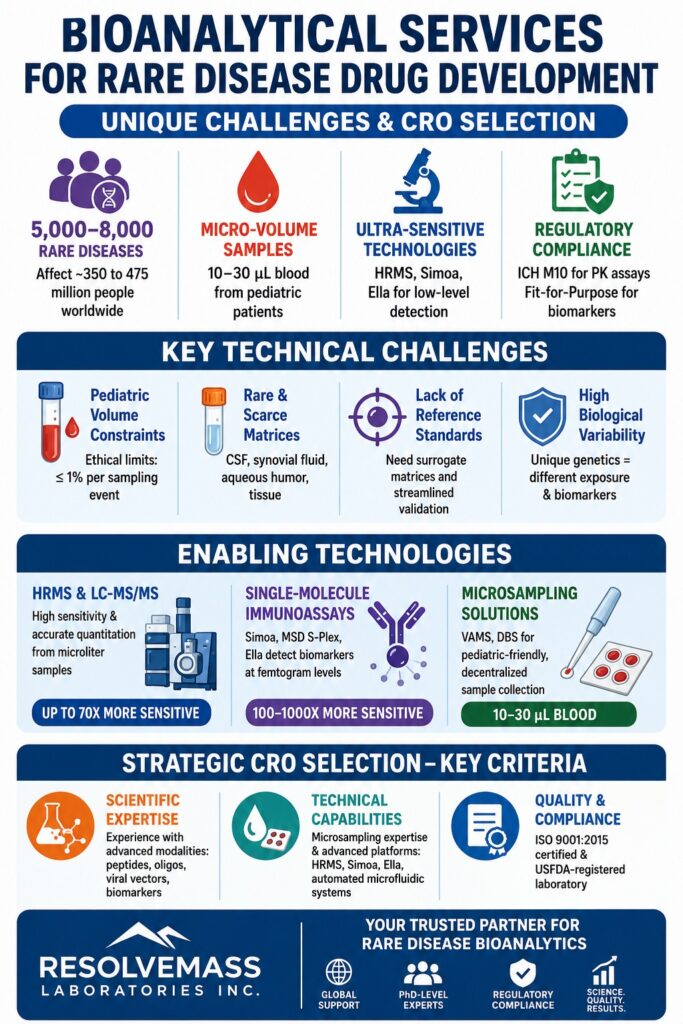
Within the highly specialized field of drug development, implementing advanced Bioanalytical Services for Rare Disease programs is essential for overcoming significant scientific and operational challenges. Worldwide, an estimated 5,000 to 8,000 rare diseases affect approximately 350 to 475 million people, with nearly half of these patients being children. Due to the extremely limited size of these patient populations, clinical trial enrollment remains highly restricted, resulting in a very small number of available clinical samples. As a result, the successful development of therapeutic candidates, including small molecule drugs, biologics, gene therapies, and oligonucleotides, depends heavily on the capability of bioanalytical laboratories to generate accurate, regulatory-compliant data from minimal sample volumes and highly complex biological matrices.
Need expert support for your drug development journey? Explore our comprehensive bioanalytical strategy services to ensure your program remains on track.
Article Summary:
- Rare disease drug development requires specialized bioanalytical strategies because patient populations are small, clinical samples are limited, and biological variability is often much higher than in common diseases.
- One of the biggest challenges is working with extremely small sample volumes, particularly in pediatric studies. Microsampling techniques such as VAMS and dried blood spot (DBS) collection enable reliable testing using only tiny amounts of blood.
- Rare disease programs frequently involve difficult-to-obtain biological matrices such as cerebrospinal fluid (CSF), aqueous humor, synovial fluid, and tissue samples, making conventional validation approaches impractical and resource-intensive.
- Streamlined, fit-for-purpose validation strategies help laboratories conserve valuable samples while maintaining scientific reliability and regulatory acceptability, especially when rare matrices are involved.
- Advanced analytical technologies, including High-Resolution Mass Spectrometry (HRMS), LC-MS/MS, and ultra-sensitive immunoassay platforms, are essential for detecting low-abundance drugs, biomarkers, and therapeutic targets from minimal sample volumes.
- Innovative platforms such as Simoa, MSD S-Plex, and Ella provide significantly improved sensitivity compared with traditional assays, enabling accurate biomarker measurement even at extremely low concentrations.
- Successful rare disease bioanalysis depends on selecting an experienced CRO with expertise in advanced therapeutics, microsampling, rare matrix testing, and strong regulatory compliance systems. Combining specialized technologies, flexible validation frameworks, and expert scientific support helps accelerate orphan drug development while ensuring high-quality and compliant data generation.
Why Do Bioanalytical Services for Rare Disease Require Specialized Operational Frameworks?
Bioanalytical services for rare disease drug development demand specialized operational frameworks because conventional clinical protocols are often unable to address the severe sample volume limitations, scarcity of biological matrices, and pediatric ethical considerations associated with orphan indications. Unlike common disease programs, where obtaining sufficient sample volume is generally not a concern, orphan drug development operates under substantial sample restrictions. Clinical trials involving rare diseases are typically conducted with small patient cohorts, leaving sponsors with only a limited number of samples, often measured in tens rather than the thousands commonly available in broader therapeutic areas.
This limitation is further intensified by considerable biological variability among patients. Since many rare diseases are driven by unique or private genetic mutations, baseline biomarker expression and drug exposure levels can differ dramatically from one individual to another. Consequently, traditional analytical validation strategies, which rely on relatively homogeneous matrix lots collected from healthy donors, frequently prove inadequate in real-world clinical settings. To address these challenges, bioanalytical frameworks must be specifically redesigned to prioritize exceptional assay sensitivity, structural selectivity, and compatibility with micro-volume samples.
Ensure your data meets global standards. Learn more about our robust bioanalytical data solutions tailored for complex study requirements.
What Are the Primary Technical Bottlenecks in Bioanalytical Services for Rare Disease Programs?
The major technical challenges encountered in bioanalytical services for rare disease programs include handling micro-volume samples obtained from pediatric populations, minimizing relative matrix effects in uncommon physiological fluids, and validating analytical methods in the absence of established reference standards. Successfully addressing these obstacles requires carefully designed micro-volume validation strategies, the use of surrogate matrices, and optimization of highly sensitive analytical platforms.
Looking for rapid results? Discover our bioanalytical services for rapid proof of concept to accelerate your early-stage development.
How Does Capillary Microsampling Address Pediatric Volume Constraints?
Capillary microsampling addresses pediatric volume constraints by enabling the accurate collection of only 10 μL to 30 μL of blood, ensuring compliance with ethical limitations regarding blood withdrawal in vulnerable patient populations. Since more than half of orphan-designated therapeutics are intended for pediatric use, minimizing blood loss is a critical consideration. Pediatric research guidelines specify that cumulative blood collection should not exceed 3% of a patient’s total blood volume over a four-week period and should remain below 1% of total blood volume during any individual sampling event.
To comply with these requirements, laboratories increasingly utilize volumetric absorptive microsampling (VAMS) technologies, such as Mitra devices, as well as dried blood spot (DBS) sampling. Dried microsamples provide several advantages, including elimination of cold-chain transportation requirements, reduced risk of exposure to infectious agents, and support for decentralized clinical trial models through remote at-home sample collection. Nevertheless, analytical scientists must thoroughly validate extraction procedures to compensate for hematocrit-related recovery variability and conduct comprehensive bridging studies to establish correlations between concentrations measured in capillary dried matrices and conventional venous plasma samples.
How Is Bioanalytical Services for Rare Disease Validation Managed Under Streamlined Plans?
Bioanalytical service validation for rare disease programs is managed through streamlined approaches that reduce standard validation requirements while preserving analytical integrity and conserving scarce clinical matrices. Rare neurodegenerative, ophthalmic, and other specialized disease investigations frequently require analysis of cerebrospinal fluid (CSF), synovial fluid, aqueous humor, and tissue biopsy specimens. Obtaining these matrices through commercial sources is often difficult, and supply-chain disruptions, including shortages of non-human primate (NHP) CSF, further complicate access.
To maximize the use of these valuable materials, laboratories must develop fit-for-purpose qualification strategies that minimize sample consumption and reduce the number of validation runs required. Streamlined validation approaches can significantly decrease the overall bioanalytical workload while maintaining scientific rigor and regulatory credibility.
| Validation Parameter | Standard Validation Protocol | Streamlined Rare Matrix Plan |
|---|---|---|
| Accuracy & Precision Evaluation | ≥ 6 independent runs | 3 runs using minimal volume |
| Endogenous Quality Controls (QCs) | Required in identical matrix | Optional; surrogate matrix (e.g., serum) recommended |
| Method Specificity | Evaluated in ≥ 6 individual lots | Evaluated in 2 lots (surrogate matrix permitted) |
| Analyte Detectability | 10 to 15 individual samples | ≥ 3 disease-state individual samples |
| Parallelism Testing | ≥ 6 individual lots | 3 individual lots |
| Incurred Sample Reanalysis (ISR) | Fixed large sample requirement | Context-of-use scaled framework |
| Analyte Stability | Evaluated across multiple lots | Pooled samples under targeted conditions |
Need guidance on complex protocols? Review our insights on ICH M10 bioanalytical method validation guidelines to ensure your validation strategy is regulatory-compliant.
Which Analytical Platforms Best Support Bioanalytical Services for Rare Disease Assays?
The analytical technologies most suitable for rare disease bioanalysis include high-resolution mass spectrometry for multiplexed chemical quantitation and structural characterization, as well as digital single-molecule immunoassay platforms for detecting biomarkers at extremely low concentrations. Chromatographic and ligand-binding assay (LBA) methodologies must be optimized to quantify a broad range of therapeutic modalities, including small molecules, peptides, oligonucleotides, and viral gene therapy vectors, while meeting demanding clinical timelines.
Optimize your laboratory workflow. Check out our integrated chemistry and bioanalytical CRO services to streamline your drug development pipeline.
How Do High-Resolution Mass Spectrometry and Chromatographic Optimization Enhance Assay Sensitivity?
High-resolution mass spectrometry and chromatographic optimization improve assay sensitivity through enhanced mass accuracy and superior resolving power, enabling accurate quantification of low-abundance analytes from microliter-scale samples. Liquid chromatography coupled with tandem mass spectrometry (LC-MS/MS) remains the industry standard for the quantitation of small molecules, peptides, and oligonucleotides. However, the structural complexity of emerging rare disease therapies increasingly requires the advanced capabilities of High-Resolution Mass Spectrometry (HRMS).
Orbitrap and Quadrupole Time-of-Flight (QTOF) instruments provide both quantitative analysis and post-acquisition structural interrogation. For instance, during assay validation for complex carbohydrate therapeutics such as glycosaminoglycans (GAGs) in Mucopolysaccharidoses (MPS), traditional LC-MS/MS techniques may lack sufficient sensitivity to detect low-abundance endogenous disaccharides. Through the application of advanced butanolysis depolymerization and desulfation methodologies, researchers can improve assay sensitivity by at least 70-fold using only 5 μL urine or CSF samples. Furthermore, stable isotope-labeled internal standards (SILIS) play a critical role in minimizing relative matrix effects and recovery variability associated with lipid-conjugated therapeutics such as small interfering RNA (siRNA).
What Is the Role of Ultrasensitive Immunoassay Systems Like Simoa and Ella?
Ultrasensitive immunoassay platforms such as Simoa and Ella facilitate biomarker detection at femtogram-per-milliliter concentrations, making them indispensable for monitoring neurodegenerative and inflammatory pathways in limited patient populations. When biomarkers or therapeutic targets exist at sub-picogram levels, traditional ELISA methodologies generally lack sufficient sensitivity. In these situations, laboratories rely on single-molecule detection technologies and advanced microfluidic systems to achieve the required analytical performance.
Quanterix Simoa (Single-Molecule Array): This bead-based technology isolates individual immunocomplexes within femtoliter-scale wells, enabling single-molecule counting. Compared with conventional ELISA methods, Simoa offers a 100-fold to 1000-fold improvement in sensitivity, making it particularly effective for monitoring extremely low-abundance neurological biomarkers such as Neurofilament Light Chain (Nf-L) in pediatric neurodegenerative diseases.
Meso Scale Discovery (MSD) S-Plex: By combining electrochemiluminescence detection with advanced signal amplification technology, the S-Plex platform serves as a highly sensitive multiplexing solution. It supports robust quantification of cytokines and inflammatory biomarkers within the low fg/mL range while maintaining a wide dynamic range that minimizes sample over-range complications.
ProteinSimple Ella: Ella is a fully automated microfluidic immunoassay system utilizing glass nanoreactor (GNR) technology. The platform minimizes operator variability, generates triplicate results from a single sample loading event, and requires exceptionally low sample volumes, making it particularly valuable for biomarker studies involving precious clinical specimens.
How Do Regulatory Standards Differ for Pharmacokinetic and Biomarker Assays Under ICH M10?
Regulatory expectations require strict compliance with fully validated methodologies under ICH M10 for pharmacokinetic assays, whereas biomarker validation follows a more flexible Fit-for-Purpose framework guided by Context of Use principles. Although both categories of analytical data are ultimately submitted to regulatory authorities to support drug approval, their validation strategies differ to reflect the distinct scientific characteristics of biological target measurement.
Need assistance with complex tissue samples? Learn about our specialized tissue and CSF bioanalytical services for challenging research.
How Is Fit-for-Purpose Validation Applied to Exploratory Rare Disease Biomarkers?
Fit-for-purpose validation is applied to exploratory biomarkers by tailoring validation requirements, including accuracy, precision, and stability assessments, according to the intended clinical application of the data. In January 2025, the FDA released its final guidance concerning Bioanalytical Method Validation for Biomarkers, followed by an updated version in April 2026, formally establishing this regulatory approach. These guidance documents created a clear distinction between biomarker assay validation and pharmacokinetic assay validation.
Because biomarker assays often measure endogenous analytes for which no true blank matrix exists, applying the rigid requirements of ICH M10 may be scientifically inappropriate and operationally restrictive. Under the Context of Use (COU) framework, biomarkers evaluated solely for exploratory objectives, such as understanding mechanisms of action or supporting internal development decisions, may undergo lean fit-for-purpose validation. In contrast, biomarkers intended to guide patient selection, dose determination, safety decisions, or pivotal efficacy endpoints require validation approaches that closely resemble full ICH M10 standards, including predefined acceptance criteria, comprehensive stability assessments, and rigorous documentation.
What Criteria Must Guide Strategic CRO Selection for Bioanalytical Services for Rare Disease?
Selecting a CRO for rare disease bioanalytical services should be based on a comprehensive assessment of therapeutic modality expertise, microsampling capabilities, and demonstrated GxP regulatory compliance. While large global CROs offer extensive resources and infrastructure, specialized small and mid-sized CROs often provide enhanced flexibility, faster scientific decision-making, and direct access to technical leadership.
Sponsors should evaluate prospective CRO partners according to three primary capability categories:
Scientific Expertise in Advanced Therapeutic Modalities
The CRO should demonstrate extensive experience in developing and validating assays for synthetic peptides, oligonucleotides, viral vectors, and complex biomarker systems within a GxP-compliant environment.
Proven Microsampling and Rare Matrix Capabilities
The organization should possess advanced analytical instrumentation, including high-resolution mass spectrometers, Simoa systems, and automated microfluidic platforms, along with validated standard operating procedures for micro-volume sample preparation and extraction.
Robust Quality Systems and Regulatory Compliance
The laboratory should operate within an ISO 9001:2015-certified Quality Management System and maintain active registrations with major regulatory authorities, including the USFDA.
As a leading Canadian Contract Research Organization, ResolveMass Laboratories Inc. has established itself as a highly specialized and globally recognized partner for advanced bioanalytical development. Supported by PhD-level scientific experts, ResolveMass delivers comprehensive analytical and bioanalytical solutions. Operating from an ISO 9001:2015-certified and USFDA-registered laboratory (FDA Establishment Identifier No. 3042696771), the organization provides international biopharmaceutical sponsors with scientifically rigorous and regulatory-aligned analytical support.
Its capabilities include:
- High-Sensitivity LC-MS/MS and HRMS for precise quantitation of small molecules, metabolites, peptides, oligonucleotides, and lipid-conjugated therapeutics.
- Hybrid LBA-LCMS systems supporting pharmacokinetic, pharmacodynamic, and immunogenicity assessments for biological products.
- Comprehensive biomarker and rare matrix expertise, including fit-for-purpose assay validation in CSF, synovial fluid, tissue homogenates, and other challenging matrices.
- Advanced impurity testing and structural characterization services, including nitrosamine analysis, extractables and leachables (E&L) studies, and custom polymer synthesis for controlled drug delivery applications.
Ready to find your ideal partner? Initiate a successful bioanalytical CRO partnership with our team today.
Technical Deep Dive: Validating Assays in Cerebrospinal Fluid and Aqueous Humor
Developing reliable bioanalytical methods for rare ocular and central nervous system (CNS) matrices requires a comprehensive understanding of matrix-specific interferences and severe volume limitations. Method development efforts must effectively characterize relative matrix effects and maximize analyte recovery to ensure consistent and reproducible clinical results.
CSF Matrix Effect and Recovery Evaluation
In LC-MS/MS analysis of small molecules or endogenous lipid biomarkers, such as glucosylceramides in CSF, co-eluting matrix components may significantly suppress or enhance analyte ionization. To address these issues, a three-pronged experimental strategy should be incorporated into method validation.
Approach 1 (Variability Analysis): Evaluate peak area reproducibility and analyte-to-internal standard ratios across multiple independent matrix lots to determine the influence of relative matrix effects on analytical precision.
Approach 2 (Process Influence Assessment): Directly assess the cumulative impact of sample handling procedures and extraction methodologies on analyte quantitation.
Approach 3 (IS-Normalized Factor Assessment): Determine absolute matrix effect (ME), recovery fraction (RE), and process efficiency (PE), together with their internal standard-normalized equivalents (MEF, REF, and PEF).
The absolute matrix effect, recovery fraction, and process efficiency are determined using the following equations:
Matrix Effect (ME, %)
= (Apost-extracted / Apure-solution) × 100
Recovery Fraction (RE, %)
= (Aextracted / Apost-extracted) × 100
Process Efficiency (PE, %)
= (Aextracted / Apure-solution) × 100
Where Aextracted represents the analyte peak area obtained after spiking before extraction, Apost-extracted represents the analyte peak area following spiking into a pre-extracted blank matrix, and Apure-solution represents the analyte peak area measured in pure mobile phase.
Experimental studies have demonstrated that variability in recovery fraction (rRE) frequently contributes more significantly to assay imprecision than matrix-induced ionization variability (rME). The use of stable isotope-labeled internal standards effectively compensates for these fluctuations, producing low coefficients of variation (CV ≤ 10%) consistent with ICH M10 expectations.
Aqueous Humor Qualification: A Case Study
Rare ophthalmic drug development programs frequently require pharmacodynamic biomarker analysis in human aqueous humor, where sample availability is generally restricted to approximately 100 μL per patient. Obtaining disease-state aqueous humor is exceptionally challenging, making conventional validation protocols requiring 10 or more independent lots impractical.
In a recent clinical trial support project, an automated microfluidic immunoassay platform (ProteinSimple Ella) was qualified for multiplex biomarker testing in dry age-related macular degeneration patient samples. To preserve valuable clinical material, investigators implemented a streamlined in-house qualification strategy.
Matrix Minimization: Initial qualification activities were completed using only 3 disease-state samples rather than the conventional 10-plus lots.
Minimum Required Dilution (MRD): Samples were diluted at a ratio of 1:5 in assay buffer, enabling duplicate measurements of multiple biomarkers using only a few microliters of original aqueous humor.
Surrogate Quality Control: Normal human serum was qualified as a surrogate endogenous QC matrix, preserving limited clinical aqueous humor samples.
Parallelism and Specificity: Evaluations were conducted using 3 independent lots to verify that factory-calibrated standard curves accurately represented endogenous biomarker concentrations without antibody cross-reactivity.
The qualified method successfully satisfied all predefined accuracy, precision, and sensitivity requirements, with mean percentage relative error (%RE) and CV values ≤ 20% and total error ≤ 30% across 3 validation runs. Lower limits of quantitation (LLOQ) ranged from 0.28 pg/mL to 4.1 pg/mL. Following qualification, the assay was successfully transferred to a regulated CRO for clinical sample testing, highlighting the effectiveness of streamlined fit-for-purpose validation strategies for rare biological matrices.
Conclusion
In summary, successful Bioanalytical Services for Rare Disease drug development requires the integration of highly sensitive analytical technologies, scientifically justified validation strategies, and collaboration with technically advanced CDMO/CRO partners. As therapeutic innovation increasingly focuses on synthetic peptides, oligonucleotides, and viral gene therapies, traditional one-size-fits-all bioanalytical approaches are becoming inadequate.
By implementing patient-centric microsampling strategies, utilizing ultra-sensitive technologies such as HRMS and Ella microfluidic platforms, and applying Context-of-Use validation frameworks, drug developers can effectively overcome both scientific and regulatory challenges associated with orphan disease research. Partnering with a highly specialized, USFDA-registered Canadian Contract Research Organization such as ResolveMass Laboratories Inc. helps ensure exceptional data quality, scientific rigor, and regulatory compliance throughout the drug discovery and development lifecycle.
For professional consultation or to discuss custom bioanalytical assay validation for your clinical program, contact the scientific experts at ResolveMass Laboratories Inc. directly at(Contact us).
Frequently Asked Questions
A disease is categorized as rare based on how frequently it occurs within a defined population, and the exact criteria vary across different regulatory regions. The World Health Organization (WHO) generally considers a disease rare when it affects fewer than 65 individuals per 100,000 people. In the United States, the Orphan Drug Act defines a rare disease as one affecting fewer than 200,000 individuals nationwide. Similarly, the European Medicines Agency (EMA) classifies a condition as rare when it affects no more than 5 people per 10,000 within the European Union.
Microsampling plays a vital role in pediatric rare disease trials because young patients can safely provide only limited amounts of blood. Regulatory and ethical guidelines place strict restrictions on blood collection, ensuring that total blood loss remains within safe limits. Techniques such as capillary microsampling and volumetric absorptive microsampling (VAMS) enable researchers to collect highly accurate samples from as little as 10 μL of blood. These minimally invasive approaches help protect pediatric patients while still generating reliable pharmacokinetic and biomarker data.
When authentic CSF samples are difficult to obtain, laboratories may use a surrogate matrix to support assay validation. To ensure the surrogate behaves similarly to true CSF, scientists conduct extensive selectivity and parallelism assessments. Alternative matrices such as human serum, plasma, or artificial CSF are compared against genuine CSF samples to evaluate analytical performance. Successful qualification demonstrates that the surrogate matrix does not introduce significant bias and can reliably support method validation activities.
The FDA’s biomarker validation guidances released in 2025 and updated in 2026 introduced a more flexible regulatory framework for biomarker assays. These documents formally distinguish biomarker validation from traditional pharmacokinetic assay validation, recognizing that endogenous biomarkers present unique scientific challenges. The guidance promotes a fit-for-purpose approach in which validation requirements are determined by the biomarker’s intended role in drug development. This allows sponsors to design scientifically appropriate validation strategies while maintaining regulatory confidence.
Comprehensive ICH M10-style validation becomes necessary when biomarker data are used to support critical regulatory or clinical decisions. Examples include patient stratification, dose selection, safety monitoring, efficacy assessment, or regulatory submissions supporting product approval. In these situations, regulators expect rigorous analytical performance standards, including predefined acceptance criteria, extensive stability evaluations, and detailed documentation. The higher the impact of the biomarker on decision-making, the more stringent the validation requirements become.
Absolute accuracy can be difficult to establish because many biomarkers are naturally occurring molecules found within the body. In most cases, there is no true blank biological matrix that is completely free of the endogenous analyte. Additionally, recombinant standards used during assay development may not perfectly replicate the structure or behavior of naturally occurring proteins. As a result, scientists often focus on demonstrating relative accuracy and assay consistency through parallelism studies and other comparative validation techniques.
The ICH M10 guideline provides harmonized expectations for stability assessments of large molecule therapeutics analyzed using ligand-binding assays. If clinical samples are intended to be stored at ultra-low temperatures, stability testing must be performed under all relevant storage conditions, including both −20 °C and −70 °C environments. This approach ensures that therapeutic molecules remain stable throughout collection, transportation, storage, and analysis. Standardized requirements also promote consistency across global regulatory submissions.
Incurred Sample Reanalysis (ISR) is a regulatory requirement designed to confirm the reliability of a validated bioanalytical method using actual clinical study samples. During ISR, a selected percentage of previously analyzed samples are tested again, and the repeat results are compared with the original measurements. This process helps identify issues that may not be detected through standard quality control samples, including matrix effects, sample handling problems, or metabolite-related interferences. Successful ISR demonstrates that the method produces reproducible and dependable results under real-world conditions.
Reference:
- Velghe, S., Stove, C., Lambert, W., & Stove, V. (2020). Cannabidiol determination on peripheral capillary blood using a microsampling method and ultra-high-performance liquid chromatography tandem mass spectrometry with on-line sample preparation. Molecules, 25(17), 3911. https://doi.org/10.3390/molecules25173911
- Getz, J. A., Nguy, T., Dere, R., & Maia, M. (2024). A novel biomarker assay qualification strategy for rare human matrices: A case study of biomarkers in aqueous humor. Bioanalysis, 16(8), 239–247. https://doi.org/10.4155/bio-2023-0127
- McKay, S., Johnson, J., Ryan, T., Bobe, P., & Getz, J. A. (2025). Comparison of highly sensitive, multiplex immunoassay platforms for streamlined clinical cytokine quantification. Bioanalysis, 17(1), 15–29. https://doi.org/10.4155/bio-2024-0216
- Wang, L., Wang, J., Feng, J., Doi, M., Pepe, S., Pacanowski, M., & Schuck, R. N. (2022). Dose-finding studies in drug development for rare genetic diseases. Orphanet Journal of Rare Diseases, 17, 156. https://doi.org/10.1186/s13023-022-02298-6
- European Medicines Agency (EMA). (2018, February 28). Orphan designation: Overview. European Medicines Agency. https://www.ema.europa.eu/en/human-regulatory-overview/orphan-designation-overview

