Introduction to Dexamethasone Development Challenges
The development of sterile and stable dexamethasone injectable formulations demands careful management of numerous physical, chemical, and analytical complexities to prevent significant failures during scale-up and commercial manufacturing. Successfully overcoming these Dexamethasone Development Challenges requires stringent control of pH-dependent solubility behavior, degradation mechanisms, and interactions between the formulation and packaging components. Since dexamethasone is a highly potent corticosteroid administered directly into systemic circulation or targeted tissues, even minor variations in physical stability, chemical integrity, or sterility assurance can negatively impact patient safety and potentially result in costly product recalls.
For formulation scientists, obtaining regulatory approval from agencies such as the FDA and EMA requires a comprehensive mechanistic understanding of both the active pharmaceutical ingredient (API) and the formulation environment surrounding it. This technical guide examines the fundamental causes of development and manufacturing failures while presenting scientifically validated approaches that can effectively minimize associated risks.
Article Summary:
- Developing dexamethasone injectable formulations requires strict control of stability, sterility, and manufacturing parameters to ensure product quality, patient safety, and regulatory compliance.
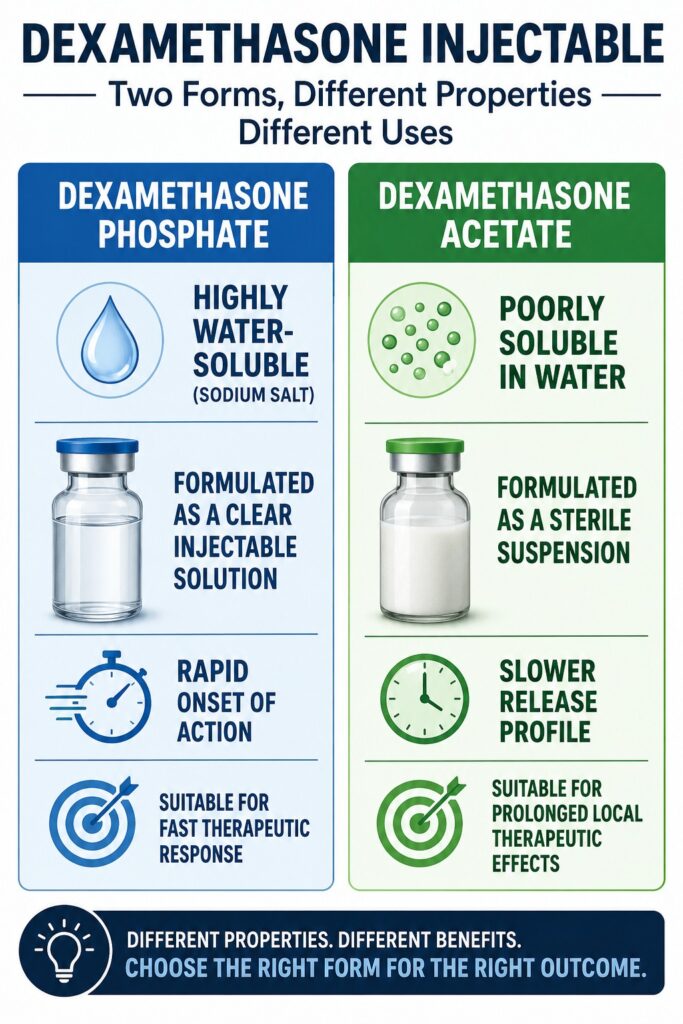
- Choosing the correct dexamethasone form is critical: dexamethasone sodium phosphate is suitable for clear injectable solutions, while dexamethasone acetate is designed for suspension formulations with prolonged therapeutic effects.
- Maintaining formulation pH between 7.0 and 8.5 is essential, as lower pH levels can trigger hydrolysis, precipitation, particulate formation, and loss of drug solubility.
- Rapid dilution of concentrated dexamethasone solutions or improper mixing with other injectable drugs can cause incompatibilities, crystallization, and reduced formulation performance.
- Chemical degradation can occur through ester hydrolysis, oxidation, light exposure, and interactions with antioxidants such as sodium bisulfite, resulting in potency loss and impurity formation.
- Manufacturing challenges include heat-induced degradation during sterilization, suspension caking, poor syringeability, and scale-up difficulties that can affect product consistency and shelf life.
- Packaging interactions and analytical limitations, including glass delamination, elastomer leachables, HPLC separation issues, hygroscopic reference standards, and UV interference from excipients, can compromise product quality and accurate testing results.
Preformulation and Physical Stability Failures
Dexamethasone Phosphate vs. Acetate: Solubility and Salt Selection Failures
Selecting either dexamethasone phosphate or dexamethasone acetate fundamentally determines whether the final dosage form will be a solution or a suspension. An inappropriate selection can lead to severe formulation failures, including phase separation, sedimentation, or irreversible caking. Dexamethasone sodium phosphate is a highly water-soluble disodium salt with solubility typically ranging from 100 to 1000 mg/mL, making it suitable for immediate-release injectable solutions. In contrast, dexamethasone acetate is a highly lipophilic ester with extremely low aqueous solubility and is therefore formulated as a suspension intended to provide prolonged local therapeutic effects through depot action.
One of the most common preformulation errors occurs when these two esters are treated as interchangeable entities without adequately considering their distinct physicochemical properties. Failure to optimize critical parameters such as particle size distribution (PSD), suspension viscosity, and sedimentation characteristics of dexamethasone acetate frequently results in thermodynamic instability, accelerated settling, and rapid phase separation during storage.
The Critical Threshold of pH-Dependent Precipitation
Maintaining a tightly controlled pH range between 7.0 and 8.5 is essential for preserving the solubility and stability of dexamethasone sodium phosphate. Any deviation below this range can trigger the rapid conversion of dexamethasone sodium phosphate into the poorly soluble free dexamethasone base. While the parent dexamethasone molecule exhibits relatively stable solubility across physiological pH conditions, the sodium phosphate ester relies heavily on a weakly alkaline environment to maintain its highly soluble ionic structure.
When the local pH falls below 7.0, acid-catalyzed hydrolysis of the phosphate ester is initiated. This reaction produces free dexamethasone, which possesses an aqueous solubility of less than 0.1 mg/mL. As a result, the active pharmaceutical ingredient can rapidly precipitate from solution, leading to visible turbidity, particulate formation, white specks, and overall loss of product quality.
Dexamethasone Sodium Phosphate (Highly Soluble, pH 7.0–8.5)
│
▼ (pH < 7.0 / Acidic Hydrolysis)
Free Dexamethasone Base (Insoluble, < 0.1 mg/mL) + Phosphate Ions
│
▼
Particulate Matter / Precipitate Formation (“Crashing Out”)
Shock Precipitation and Co-solvent Dilution Failures
Shock precipitation is a common formulation issue that occurs when concentrated organic stock solutions containing dexamethasone are diluted too rapidly into aqueous media. This process creates localized concentrations that exceed the solubility limits of the drug, resulting in immediate precipitation. Lipophilic dexamethasone derivatives, including dexamethasone acetate and dexamethasone phenylpropionate, are frequently dissolved in organic solvents such as dimethyl sulfoxide (DMSO) or ethanol to prepare high-concentration stock solutions.
When these organic solutions are introduced rapidly into aqueous buffers, the local solvent composition changes abruptly. The concentration of organic solvent decreases below the level necessary to maintain steroid solubility, causing rapid solvent exchange and instantaneous crystal formation. This precipitation process is generally irreversible and leads to aggregation and crystallization of the active ingredient. Preventing this phenomenon requires controlled addition rates, stepwise dilution procedures, high-shear mixing, and carefully regulated processing temperatures.
Co-administration and Admixture Incompatibilities
Physical incompatibility problems frequently arise when dexamethasone injectable formulations are mixed with other injectable medications before administration. Dexamethasone sodium phosphate formulations are commonly buffered with sodium citrate and maintained at a weakly basic pH. When these solutions are combined with weakly acidic local anesthetics such as bupivacaine hydrochloride or ropivacaine hydrochloride, the resulting pH shift can convert the anesthetic into its un-ionized free-base form.
This conversion significantly reduces aqueous solubility and can cause rapid crystallization and precipitation. Similar incompatibilities may occur when dexamethasone is combined with cationic antiemetic agents such as ondansetron. In such cases, molecular charge neutralization may occur, resulting in the formation of insoluble drug-drug complexes that precipitate from solution and compromise the safety and effectiveness of the admixture.
Chemical Degradation Pathways
Active Ester Hydrolysis and Active Drug Loss
The primary mechanism responsible for potency loss in dexamethasone solutions is acid- or base-catalyzed hydrolysis of the phosphate ester linkage. The degradation process follows first-order reaction kinetics, with the rate constant being strongly influenced by both temperature and the concentration of hydronium or hydroxide ions present within the formulation.
[
C_t = C_0 e^{-0.1769t}
]
Under non-optimal pH conditions, water molecules act as nucleophiles and attack the phosphorus atom within the phosphate ester. This reaction cleaves the C-21 ester bond and generates free dexamethasone along with inorganic phosphate ions. A frequent formulation deficiency involves inadequate buffer capacity. During dilution into clinical administration vehicles such as 0.9% sodium chloride injection or 5% dextrose injection, citrate buffer concentrations can decline from approximately 50 mM to below 3 mM. Such dilution significantly reduces buffering capacity, resulting in sudden pH changes and accelerated hydrolysis of the active ingredient.
The Antioxidant Paradox: Sodium Bisulfite and Sulfonated Impurities
The incorporation of sodium bisulfite or sodium sulfite as antioxidants in dexamethasone formulations can create serious stability concerns because these compounds are capable of reacting directly with the steroid structure. Sodium bisulfite is often included at concentrations around 1 mg/mL to minimize oxidative degradation; however, under thermal stress conditions such as autoclaving or long-term storage, it can participate in nucleophilic addition or substitution reactions with dexamethasone sodium phosphate.
These reactions generate a stable but therapeutically inactive degradation product known as dexamethasone sodium phosphate impurity I, a sulfonated derivative of the active ingredient. Because this impurity accumulates progressively during storage, batches may eventually exceed the stringent USP and ICH limits established for unspecified individual impurities, which are typically restricted to 0.10%.
Photolytic and Oxidative Side Chain Degradation
Exposure to light and dissolved oxygen significantly accelerates degradation of the dihydroxyacetone side chain of dexamethasone. Functional groups located at the C-17 and C-21 positions of the steroid nucleus are particularly susceptible to oxidative attack initiated through free-radical mechanisms.
In the presence of oxygen and light, photolytic reactions generate free radicals that attack and fragment the side chain, producing degradation products such as carbon monoxide, formaldehyde, and a variety of acidic and ketonic compounds. Formulations exposed to excessive light during manufacturing, filling, or storage often develop a characteristic yellow-to-pink discoloration. This visible color change is frequently accompanied by substantial reductions in active ingredient assay values and overall product stability.
Sterile Manufacturing and Process Scale-Up Failures
Terminal Sterilization vs. Aseptic Processing Failures
Applying conventional terminal steam sterilization to dexamethasone injectable products is often problematic due to the thermal sensitivity of the steroid molecule. Although regulatory agencies such as the FDA and EMA generally prefer terminal sterilization because it provides the highest level of sterility assurance, the process can cause unacceptable levels of chemical degradation.
The validated Sterility Assurance Level (SAL) achieved through terminal sterilization is represented as:
[
\text{SAL} = 10^{-6}
]
This value corresponds to a one-in-a-million probability that a viable microorganism survives the sterilization process.
However, standard autoclaving conditions, such as 121°C for 20 minutes, frequently provide sufficient thermal energy to accelerate ester hydrolysis and oxidative degradation pathways. Consequently, developers are often required to establish comprehensive aseptic manufacturing processes and demonstrate through detailed heat-stress and degradation studies that terminal sterilization is not chemically feasible for the product.
Suspension Caking and Syringeability Failures for Dexamethasone Acetate
Dexamethasone acetate suspensions commonly experience formulation challenges related to irreversible caking, reduced syringeability, and inconsistent dose delivery. The performance of these suspensions depends on a delicate balance among particle size, sedimentation behavior, zeta potential, and viscosity.
The crystal morphology of the active pharmaceutical ingredient has a particularly important influence on injectability. Plate-shaped or tabular crystals generally pass more easily through fine-gauge needles, whereas needle-shaped or acicular crystals are more prone to interlocking and clogging syringe openings. In addition, inadequate optimization of suspending agents such as sodium carboxymethylcellulose and polysorbate 80 can promote Ostwald ripening. During this process, smaller particles dissolve and subsequently recrystallize onto larger particles, causing progressive particle growth and eventually leading to dense, irreversible sediment formation at the bottom of the container.
Packaging-Material Interactions
Glass Delamination Induced by Weakly Alkaline Formulations
Glass delamination is a serious packaging-related failure characterized by the shedding of microscopic glass flakes from the inner surface of borosilicate containers into the drug solution. This phenomenon has been associated with numerous product recalls and is particularly relevant for dexamethasone formulations maintained within the weakly alkaline pH range of 7.0 to 8.5.
The root cause of delamination often originates during vial manufacturing. During flame-forming operations, volatile elements such as sodium and boron may evaporate from the heel region of the vial and subsequently redeposit onto adjacent surfaces. This process creates localized areas enriched in sodium borate and depleted in silica, resulting in chemically vulnerable surface regions.
During storage, the alkaline sodium citrate buffer continuously interacts with these altered surfaces. Hydrolysis of the siloxane network occurs, causing swelling, cracking, and eventual separation of thin glass layers from the interior vial surface. These detached glass lamellae are often difficult to detect through routine visual inspection but can pose significant clinical risks, including vascular blockage and inflammatory responses. Such findings frequently trigger Class I recalls by regulatory authorities.
Alkaline Buffer (pH 7.0–8.5) Attacks the Vial Surface
│
▼
Hydrolysis of the Siloxane Network at the Flame-Altered Heel Zone
│
▼
Leaching of Sodium and Boron Ions into the Solution
│
▼
Swelling and Cracking of the Inner Glass Surface
│
▼
Formation and Release of Microscopic Glass Lamellae (Delamination Flakes)
Elastomeric Closure Leachables and Sorption Failures
Interactions between dexamethasone formulations and elastomeric closures can result in either active drug loss or contamination by packaging-derived compounds. Elastomeric components, including vial stoppers and syringe plungers, consist of complex polymeric systems containing vulcanizing agents, antioxidants, plasticizers, accelerators, and numerous processing additives.
Over the product shelf life, dexamethasone molecules may adsorb onto the elastomer surface or diffuse into the bulk rubber matrix, leading to gradual reductions in drug concentration and potency. At the same time, chemical constituents from the elastomer can migrate into the formulation as leachables. These compounds may react directly with dexamethasone or interfere with stability-indicating analytical methods, resulting in failures to meet the stringent requirements established by USP standards and other regulatory guidelines.
Resolving Analytical Dexamethasone Development Challenges
HPLC Resolution Failures in Stability-Indicating Methods
Analytical failures during stability assessment often arise from the use of HPLC methods that are not truly stability-indicating. Such methods may be unable to adequately separate dexamethasone from structurally related impurities, degradation products, or stereoisomers.
Dexamethasone shares significant structural similarities with compounds such as betamethasone and delta-8(9)-dexamethasone. If chromatographic parameters including mobile-phase composition, pH, gradient profile, or column temperature are not carefully optimized, these substances may co-elute with the principal dexamethasone peak. Co-elution can mask degradation and produce artificially elevated assay values.
To avoid these issues, analytical scientists must establish robust reverse-phase HPLC methods utilizing C18 stationary phases, typically containing particle sizes between 1.7 µm and 5 µm. Properly validated water-acetonitrile gradient systems should provide a chromatographic resolution (Rs) of at least 1.5 between dexamethasone and adjacent impurity peaks.
Reference Standard Calibration Failures Due to Hygroscopicity
The use of uncorrected dexamethasone sodium phosphate reference standards is a common source of analytical error because the material is highly hygroscopic and can absorb up to 14% of its weight in water under ambient conditions.
Dexamethasone sodium phosphate readily behaves as a hydrated material when exposed to environmental humidity. If analysts prepare calibration standards based solely on gross weight without applying a dry-weight correction obtained through thermogravimetric analysis (TGA) or loss-on-drying (LOD) measurements, the actual amount of active steroid introduced into the analytical system will be lower than assumed.
This discrepancy produces calibration errors that can lead to falsely reduced assay values, often falling below the required 97.0% specification limit. As a result, otherwise compliant production batches may be subjected to unnecessary investigations and costly quality reviews.
Spectrophotometric Overlap and Stabilizer Interferences
Direct UV spectrophotometric analysis of dexamethasone injectable products is frequently complicated by spectral interference from formulation excipients and stabilizing agents. One notable example is creatinine, which is incorporated into several commercial dexamethasone sodium phosphate formulations to enhance physical stability.
Creatinine exhibits strong UV absorption characteristics that overlap significantly with the absorbance maximum of dexamethasone near 240 nm. This overlap makes direct quantitative measurement unreliable and often impossible without prior chromatographic separation.
To overcome this challenge, analytical scientists must employ advanced quantification strategies such as zero-crossing derivative spectrophotometry or validated HPLC methods. These approaches allow accurate isolation and measurement of dexamethasone while eliminating interference from creatinine and other formulation components, ensuring reliable analytical performance throughout product development and stability evaluation.
Dexamethasone Development FAQs
Dexamethasone sodium phosphate is typically formulated within a weakly alkaline pH range of 7.0 to 8.5, whereas bupivacaine hydrochloride exists in a more acidic environment. When these two solutions are combined, the resulting pH change can alter the ionization state of bupivacaine. This conversion promotes the formation of the poorly soluble free-base form of the anesthetic. As its solubility decreases, visible crystals or particulate matter may develop within the admixture, creating compatibility concerns during administration.
The appearance of white particles in dexamethasone vials is often linked to the gradual hydrolysis of dexamethasone sodium phosphate. During this degradation process, the phosphate ester group is cleaved, producing free dexamethasone. Unlike the phosphate salt, free dexamethasone has extremely limited solubility in aqueous solutions. As the concentration exceeds its solubility limit, the drug crystallizes and becomes visible as white spots, suspended particles, or sediment.
Routine autoclaving of dexamethasone sodium phosphate injection is generally avoided because the active ingredient is sensitive to elevated temperatures. Exposure to sterilization conditions such as 121°C can accelerate both hydrolytic and oxidative degradation pathways. These reactions may significantly reduce drug potency while increasing impurity levels. For this reason, aseptic manufacturing processes are often preferred when developing sterile dexamethasone injectable products.
Although sodium bisulfite is commonly used to minimize oxidative degradation, it can create additional stability challenges in dexamethasone formulations. Under conditions such as thermal processing or long-term storage, sodium bisulfite may react with the steroid structure of dexamethasone sodium phosphate. This interaction can generate sulfonated degradation products, including dexamethasone sodium phosphate impurity I. The accumulation of these impurities may negatively affect product quality, purity specifications, and shelf-life performance.
The recommended pH range for dexamethasone sodium phosphate injection is generally maintained between 7.0 and 8.5. This weakly alkaline environment helps preserve the stability and solubility of the phosphate ester. If the pH falls below 7.0, acid-catalyzed hydrolysis may occur more rapidly, while excessively alkaline conditions can encourage base-catalyzed degradation and oxidation. Maintaining the correct pH is therefore essential for long-term product stability.
Glass delamination occurs when microscopic flakes detach from the internal surface of a glass vial and migrate into the drug solution. In dexamethasone products, the weakly alkaline formulation can gradually attack vulnerable regions of borosilicate glass, particularly areas altered during the vial manufacturing process. Over extended storage periods, this chemical interaction weakens the glass surface and causes thin layers to separate. The resulting glass particles present significant quality and patient safety concerns.
Dexamethasone sodium phosphate is highly hygroscopic and readily absorbs moisture from the surrounding environment. As a result, reference standards may contain a substantial amount of water that contributes to the measured weight but not to the active drug content. If analysts fail to apply moisture corrections using techniques such as TGA or LOD, calibration standards may be inaccurately prepared. This can lead to misleading assay results and unnecessary investigations during quality control testing.
Dexamethasone phosphate and dexamethasone acetate differ significantly in their solubility and therapeutic applications. Dexamethasone phosphate is a highly water-soluble sodium salt that is typically formulated as a clear injectable solution for rapid onset of action. Dexamethasone acetate, on the other hand, is poorly soluble in water and is commonly prepared as a sterile suspension. This suspension formulation provides a slower release profile, making it suitable for prolonged local therapeutic effects.
Reference:
- Samtani, M. N., & Jusko, W. J. (2005). Stability of dexamethasone sodium phosphate in rat plasma. International Journal of Pharmaceutics, 301(1–2), 262–266. https://doi.org/10.1016/j.ijpharm.2005.06.003
- Buga, I., Uzoma, J. I., Reindel, K., Rashid, K., Diep, T., McCartan, P., & Zhao, F. (2021). Physical and chemical stability of dexamethasone sodium phosphate in intravenous admixtures used to prevent chemotherapy-induced nausea and vomiting. Hospital Pharmacy, 56(4), 215–220. https://doi.org/10.1177/0018578719888912
- Pu, P., Ye, F., & Qi, N. (2021). Dexamethasone sodium phosphate injection and preparation method thereof (China Patent No. CN113730348A). China National Intellectual Property Administration. https://patents.google.com/patent/CN113730348A/en
- Li, Y., He, Y., Li, W., & Hu, J. (2020). Dexamethasone acetate injection and preparation method thereof (China Patent No. CN106565810A). China National Intellectual Property Administration. https://patents.google.com/patent/CN106565810A/en
- Hwang, H., Park, J., Lee, W. K., Lee, W. H., Leigh, J.-H., Lee, J. J., Chung, S. G., Lim, C., Park, S. J., & Kim, K. (2016). Crystallization of local anesthetics when mixed with corticosteroid solutions. Annals of Rehabilitation Medicine, 40(1), 21–27. https://doi.org/10.5535/arm.2016.40.1.21
- Suknuntha, K., Wattanapoka, K., Poonpattanachai, P., Titipornwanich, N., & Sripakdee, W. (2022). Compatibility and physical properties of dexamethasone–ondansetron intravenous admixture. Hospital Pharmacy, 57(5), 666–672. https://doi.org/10.1177/00185787221074563
- Walker, S. E., DeAngelis, C., Iazzetta, J., & Eppel, J. G. (1991). Compatibility of dexamethasone sodium phosphate with hydromorphone hydrochloride or diphenhydramine hydrochloride. American Journal of Hospital Pharmacy, 48(10), 2161–2166.

