Introduction: The Real Test of a Bioanalytical Method Begins After Validation
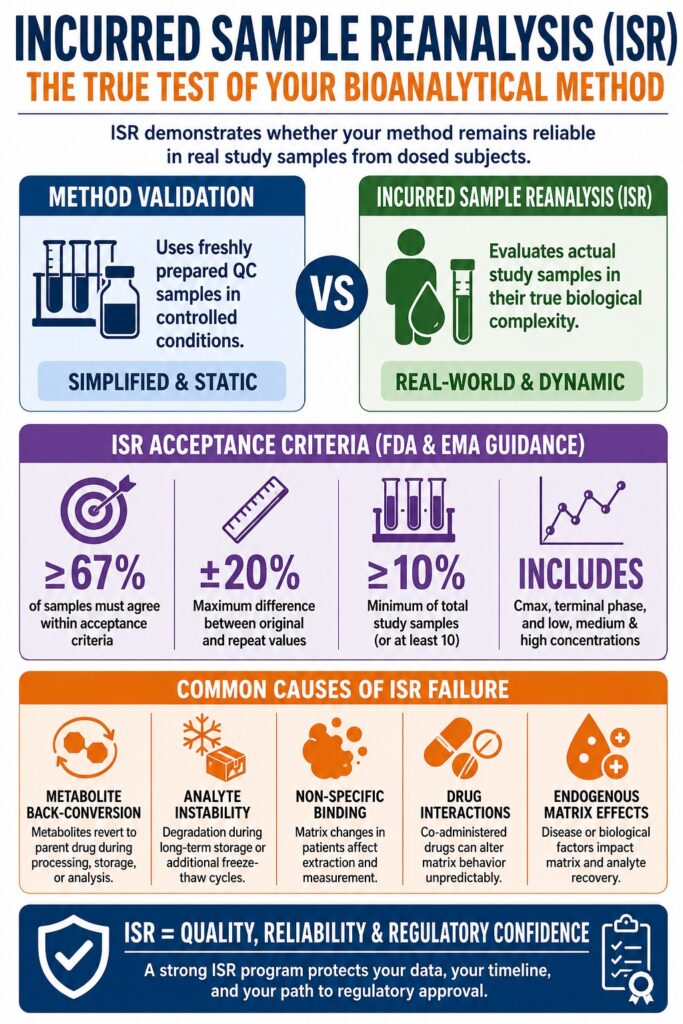
Method validation confirms that a bioanalytical method performs reliably under controlled and predefined laboratory conditions. Incurred Sample Reanalysis (ISR) in bioanalytical studies demonstrates whether that same method remains reliable within the true biological complexity of real study samples collected from dosed subjects. These are fundamentally different scientific challenges, and misunderstanding the distinction has contributed to expensive delays, regulatory deficiencies, and failed submissions throughout drug development programs.
Following the Crystal City IV Workshop in 2010, along with later FDA and EMA regulatory guidance updates, ISR evolved from a recommended practice into a regulatory expectation across nearly all pharmacokinetic (PK) studies supporting New Drug Applications (NDAs), Abbreviated New Drug Applications (ANDAs), and Biologics License Applications (BLAs). Despite this regulatory importance, many development teams still underestimate the scientific significance of ISR failures and what those failures reveal about drug behavior within biological systems.
Learn how to avoid common pitfalls in your study design: Common Bioanalytical Mistakes to Avoid
Share Via:
📌 Article Summary — Key Takeaways at a Glance
- Incurred Sample Reanalysis (ISR) is performed after initial sample analysis to verify that pharmacokinetic (PK) results obtained from real study samples can be consistently reproduced under actual biological conditions — something routine method validation alone cannot fully demonstrate.
- An ISR discrepancy is rarely just a routine laboratory mistake. In many cases, it reflects deeper scientific factors such as metabolite conversion, matrix-related interference, variability in protein binding, or analyte instability within authentic biological samples collected from treated subjects.
- Global regulatory authorities including the FDA, EMA, and Health Canada consider ISR an essential measure of bioanalytical method reliability and suitability for regulatory decision-making rather than a simple compliance formality.
- ISR performance is generally considered acceptable when at least two-thirds (67%) of repeat analyses remain within ±20% of the average between the initial and repeat result, with certain assay platforms allowing wider variability limits under specific circumstances.
- Selecting ISR samples requires scientific planning. High-risk pharmacokinetic regions such as peak concentration (Cmax) and terminal elimination phases are intentionally targeted because analytical inconsistencies are more likely to appear in these intervals.
- Significant ISR deficiencies can lead to serious regulatory consequences, including agency inspections, requests for additional data review, study reanalysis requirements, or challenges to the validity of pharmacokinetic conclusions used in submissions. Advanced bioanalytical laboratories use ISR as an ongoing analytical performance assessment tool to identify method limitations, monitor study integrity, and detect emerging issues throughout the lifecycle of a development program.
Why ISR Detects What Method Validation Cannot
Traditional method validation relies on freshly prepared quality control (QC) samples created by spiking known amounts of drug into blank biological matrix under tightly controlled conditions. ISR, in contrast, evaluates actual study samples in which the drug and its metabolites have circulated through a living biological system, creating biochemical conditions that cannot be completely reproduced in the laboratory.
A major limitation of standard validation QC samples is that they remain static and simplified. They do not replicate the constantly changing biological environment encountered by a drug after administration. In an incurred sample, analysts must account for several additional complexities, including:
Active Metabolite Species
Some metabolites may not have been incorporated into the original method development process. Certain metabolites can also interconvert with the parent compound during storage, freeze-thaw cycles, extraction, or analysis, potentially altering measured concentrations.
Plasma Protein Binding Complexity
Protein binding can vary significantly among individual subjects, influencing analyte recovery in ways that spiked QC samples cannot accurately simulate.
Co-Administered Drug Interactions
In multi-drug studies, concomitant medications may alter matrix behavior unpredictably, creating analytical effects that are absent during controlled validation experiments.
Endogenous Matrix Modifiers
Factors such as elevated bilirubin levels, abnormal lipid content, inflammatory markers, or disease-associated enzyme activity can substantially influence matrix behavior in patient populations compared with healthy volunteers.
Sample Degradation Differences
The degradation profile of an analyte in stored incurred samples may differ from freshly spiked samples because active biological enzymes and endogenous compounds remain present in the biological matrix.
Explore our approach to ensuring study reliability: Developing Robust Bioanalytical Data for Regulatory Success
ISR Acceptance Criteria: Understanding the Regulatory Thresholds
The commonly accepted ISR criterion requires that at least 67% (two-thirds) of reanalyzed samples demonstrate agreement within ±20% of the mean of the original and repeat values. Failure to meet this requirement is not considered a minor procedural issue. Instead, it indicates that the bioanalytical data supporting pharmacokinetic conclusions may lack sufficient reliability.
| Parameter | Standard ISR Criterion | Regulatory Basis | Implication of Failure |
|---|---|---|---|
| Acceptance threshold | ≥67% of samples within criteria | FDA BMV Guidance 2018; EMA 2011 | Questions reproducibility of the entire study method |
| Difference calculation | ±20% of mean of original + repeat | Crystal City IV Consensus | PK parameters such as AUC and Cmax may require recalculation |
| Sample number (small studies) | ≥10% of total samples or minimum 10 | FDA and EMA guidance | Insufficient ISR sampling weakens reproducibility assessment |
| Sample selection | Includes Cmax and terminal elimination phase | Scientific consensus | Poor selection strategy may overlook high-risk samples |
| Concentration range | Includes low, medium, and high concentrations | EMA guidance and best practice | Bias at concentration extremes may remain undetected |
| Biologic/LBA methods | ≥67% within ±30% in some cases | EMA Guideline on Bioanalytical Method Validation | Broader variability allowance reflects inherent LBA complexity |
Although the ±20% acceptance range may initially appear broad, it was intentionally established to accommodate legitimate biological variability. When repeat analyses consistently trend higher or lower than original values, the directional pattern becomes an important diagnostic indicator. A random distribution of variability differs substantially from a systematic analytical bias, and experienced bioanalytical laboratories understand how to interpret these distinctions appropriately.
Stay compliant with the latest global standards: Understanding ICH M10 Bioanalytical Method Validation Guidelines
The Scientific Causes Behind ISR Failure
ISR failure rarely results from a single isolated mistake. In most situations, it exposes a deeper structural limitation in the analytical method when applied to complex biological matrices under real study conditions. The most common causes include metabolite interconversion, analyte instability during storage, and matrix-dependent analytical effects not captured during conventional validation.
1. Metabolite Back-Conversion
Metabolite back-conversion represents one of the most scientifically important ISR failure mechanisms. Certain metabolites, especially acyl glucuronides, N-oxides, and sulfate conjugates, may revert back to the parent compound during extraction, processing, storage, or chromatographic analysis. Freshly prepared QC samples do not contain these active metabolites and therefore cannot reproduce this behavior.
In incurred samples, however, metabolites may exist at substantial concentrations. Minor changes in analytical conditions, extraction timing, or instrument performance between original and repeat analyses can alter the rate of back-conversion. As a result, the same stored aliquot may appear to contain different parent drug concentrations during ISR.
A common diagnostic pattern involves ISR values trending consistently higher than original measurements across multiple subjects and time points, especially during later pharmacokinetic phases where metabolite-to-parent ratios are elevated.
2. Analyte Instability During Long-Term Storage
ISR is generally performed after the initial sample analysis phase has been completed. Consequently, incurred samples often experience additional freeze-thaw cycles and extended storage durations at −70°C or −20°C beyond those evaluated during standard validation studies.
If the analyte exhibits only marginal long-term stability under these conditions, ISR commonly reveals a systematic decrease in repeat concentrations relative to the original values. This issue is particularly relevant for peptide therapeutics, oligonucleotides, and oxidation-sensitive small molecules.
Ensure your samples remain viable throughout the study lifecycle: Best Practices for Bioanalytical Stability Testing
3. Non-Specific Binding in Complex Biological Matrices
Certain patient populations, including subjects with hepatic impairment, renal dysfunction, or inflammatory disease states, may possess unusually high concentrations of acute-phase proteins, lipids, or uremic toxins. These matrix alterations can significantly affect non-specific binding behavior during extraction or chromatographic analysis.
As a result, concentration-dependent ISR failures may emerge that are difficult to identify without a detailed evaluation across different patient subgroups and clinical conditions.
Expert Observation
ISR failures occurring primarily at low concentrations near the lower limit of quantification (LLOQ) often indicate a completely different root cause compared with failures concentrated near the upper limit of quantification (ULOQ). Recognizing this distinction is essential during ISR investigations, as it directly influences the corrective analytical strategy and determines whether revalidation is necessary.
Strategic ISR Sample Selection: Why True Randomness Is Rare
An effective ISR strategy does not rely on purely random sample selection. Instead, it intentionally targets time points and subject profiles where analytical stress is greatest, including the Cmax region, terminal elimination phase, and pharmacokinetic outliers. These areas are where method weaknesses are most likely to become apparent.
A scientifically robust ISR selection plan should consider the following factors:
Pharmacokinetic Phase Coverage
Samples from both absorption and elimination phases ensure that the method is challenged across the complete dynamic concentration range observed during the study.
Metabolite-Rich Time Points
Late-stage samples, where metabolite concentrations exceed parent drug levels, represent the highest risk for metabolite back-conversion and related analytical interference.
Subject Diversity
Including subjects with unusually high or low exposure profiles helps evaluate method performance across the full range of biological variability.
Multiple-Dose Studies
Steady-state samples from repeat-dose studies require separate ISR representation because accumulation effects and enzyme induction may significantly alter matrix composition.
Special Population Cohorts
Dedicated ISR sampling should be performed for hepatic impairment, renal impairment, or other special population studies rather than relying solely on inclusion within the general sample pool.
Accelerate your early-phase programs with strategic support: Bioanalytical Support for IND-Enabling Studies
ISR Across Different Bioanalytical Platforms: LC-MS/MS vs. Ligand Binding Assays
ISR applies to both LC-MS/MS methods for small molecules and ligand binding assays (LBAs) used for biologics. However, the causes of ISR failure, acceptance ranges, and data interpretation differ considerably because of the distinct physicochemical properties of these analytes.
| Feature | LC-MS/MS (Small Molecules) | Ligand Binding Assays (Biologics) |
|---|---|---|
| ISR acceptance criterion | ±20% of mean | ±30% of mean in some EMA contexts; ±20–30% varies by agency |
| Primary ISR failure mechanism | Metabolite back-conversion and extraction variability | Anti-drug antibody interference, receptor occupancy, hook effect |
| Matrix effect concern | Ion suppression or enhancement from co-eluting compounds | Non-specific binding, matrix viscosity, complement activation |
| Stability-related ISR impact | Chemical degradation and metabolite conversion | Aggregation, denaturation, target-mediated binding |
| Critical ISR timing | Terminal elimination phase | Trough concentrations where ADA interference is greatest |
Specialized services for complex large molecule analysis: Advanced Proteomics Bioanalytical Services
Regulatory Consequences of ISR Non-Compliance
Poor ISR documentation or unresolved ISR failures within regulatory submissions can lead to Complete Response Letters (CRLs), clinical hold escalations, or demands for complete bioanalytical resubmission. These setbacks can extend drug approval timelines by 12 to 24 months.
The FDA’s 2018 Bioanalytical Method Validation Guidance clearly states that ISR results must be included in regulatory submissions, and failure to conduct ISR is itself considered a deficiency.
Potential regulatory consequences include:
Deficiency Letters
Regulatory agencies may request detailed ISR investigation reports and corrective action documentation before allowing the submission process to continue.
Bioequivalence Study Invalidation
In ANDA submissions, excessive ISR failure rates in bioequivalence studies may invalidate the study entirely and require complete clinical repetition.
For-Cause Inspections
Unexpected ISR anomalies may trigger inspections of bioanalytical facilities, including extensive review of raw data integrity, traceability, and SOP compliance.
Mandatory Reanalysis
Regulators may require full reanalysis of all study samples using a revised and revalidated analytical method, creating substantial financial and timeline burdens.
- ≥67%
Minimum ISR pass rate required by FDA and EMA guidance - ±20%
Maximum acceptable difference between original and repeat concentrations - 10%
Minimum percentage of total study samples typically required for ISR - 3×
Recommended minimum freeze-thaw survivability for incurred samples under ISR best practices
Ensure your data stands up to regulatory scrutiny: Maintaining Data Integrity in Bioanalytical Studies
How Advanced Bioanalytical Laboratories Use ISR as a Scientific Intelligence Tool
Beyond satisfying regulatory requirements, a comprehensive ISR program can provide valuable scientific insight into drug behavior within biological systems. ISR findings may influence formulation strategies, dosing regimens, metabolite monitoring plans, and long-term development decisions.
At ResolveMass Laboratories Inc., ISR is treated not merely as a compliance exercise but as a scientific diagnostic framework.
Systematic Trend Analysis Across Subjects and Time Points
Careful trend evaluation helps determine whether ISR discrepancies are random or linked to specific subjects, concentration ranges, or pharmacokinetic phases. Each pattern may indicate a distinct analytical issue.
Metabolite Monitoring During ISR Runs
Correlating parent drug variability with metabolite exposure profiles enables earlier identification of clinically meaningful metabolite conversion pathways.
Cross-Study ISR Performance Monitoring
Long-term ISR trend tracking across multiple studies can identify gradual analytical drift associated with column aging, reagent variability, or instrument calibration changes before major study-level failures occur.
Integration of ISR with Stability Programs
When ISR failures occur alongside marginal freeze-thaw stability results, laboratories can proactively modify storage procedures and sample handling workflows to protect ongoing studies.
Discover how we support rapid clinical transitions: Bioanalytical Services for Rapid Proof of Concept
Conclusion: ISR Represents the True Fitness-for-Purpose Assessment
In bioanalytical science, method validation marks the beginning of analytical evaluation rather than the endpoint. Incurred Sample Reanalysis (ISR) is the stage where an analytical method encounters the full complexity of biological reality, including metabolite burden, heterogeneous matrices, variable protein binding, and cumulative storage-related effects that cannot be replicated using spiked QC samples alone.
A well-designed ISR program built upon strategic sample selection, structured failure investigation, and platform-specific expertise represents one of the most valuable risk-management investments within modern drug development.
ISR failures should not automatically be viewed as laboratory mistakes. Instead, they are biological signals that provide insight into the interaction between the analytical method and the real-world biological matrix. The distinction between laboratories that simply attempt to correct ISR failures and those that scientifically interpret them ultimately defines the difference between reactive compliance and true analytical excellence.
Partner with experts to ensure seamless method performance: The Benefits of a Strategic Bioanalytical CRO Partnership
At ResolveMass Laboratories Inc., this scientific depth and interpretive rigor are integrated into every bioanalytical study, helping ensure that pharmacokinetic data remains not only compliant but also scientifically defensible throughout every regulatory milestone.
Frequently Asked Questions (FAQs)
ISR is important because pharmacokinetic conclusions depend entirely on the accuracy of concentration data generated during sample analysis. Even a validated analytical method may behave differently when exposed to complex biological samples from actual subjects. ISR verifies whether the method remains consistent across different analytical runs and storage conditions. Without ISR, there is a greater risk that PK parameters such as AUC, Cmax, and half-life could be based on inaccurate or non-reproducible data.
The standard ISR acceptance criterion requires that at least 67% of repeat sample results fall within ±20% of the mean of the original and repeated values. For some biologic assays, regulatory agencies may allow wider limits such as ±30% because of the inherent variability of ligand binding assays. These criteria are designed to account for normal biological and analytical variability while still ensuring method consistency. Failure to meet the acceptance threshold may trigger additional investigations or method reassessment.
ISR samples are not selected randomly without scientific consideration. Analysts typically choose samples from critical pharmacokinetic phases, including peak concentration points and terminal elimination phases. Samples representing low, medium, and high concentration ranges are also included to challenge the method across its entire working range. In many studies, samples from subjects with unusual PK profiles are intentionally selected because they may reveal hidden analytical weaknesses.
ISR failure can occur for several scientific reasons, including metabolite back-conversion, analyte instability during storage, matrix effects, or inconsistent extraction recovery. In some cases, disease-related biological components such as lipids or proteins interfere with the analytical process. Long-term storage and repeated freeze-thaw cycles may also alter analyte stability differently in incurred samples than in spiked QC samples. These failures often indicate limitations in how the method performs under real biological conditions.
Metabolite back-conversion occurs when a drug metabolite transforms back into the parent compound during sample handling, extraction, or analysis. This phenomenon is particularly common with unstable metabolites such as acyl glucuronides or sulfate conjugates. Because freshly prepared QC samples usually do not contain active metabolites, traditional validation studies may not detect this issue. ISR often reveals back-conversion through consistently higher repeat concentrations compared with the original analytical results.
Method validation evaluates analytical performance under controlled laboratory conditions using prepared QC samples, while ISR evaluates performance using real study samples from dosed subjects. Validation confirms parameters such as accuracy, precision, selectivity, and stability in a simplified environment. ISR, however, challenges the method under actual biological conditions that include metabolites, endogenous compounds, and subject-specific matrix variability. Together, validation and ISR provide a more complete assessment of method reliability.
ISR is commonly required in pharmacokinetic, bioequivalence, toxicokinetic, and clinical biomarker studies that support regulatory submissions. Both small molecule LC-MS/MS assays and large molecule ligand binding assays are subject to ISR expectations. Studies involving biologics, peptides, oligonucleotides, and complex metabolites may require even more careful ISR evaluation because of higher biological variability. Regulatory agencies generally expect ISR whenever bioanalytical data are used to support critical clinical or regulatory decisions.
Reference:
- National Library of Medicine. (2011). PubMed record for PMID: 21545349. PubMed. https://pubmed.ncbi.nlm.nih.gov/21545349/
- Chongwoo Yu & E Dennis Bashaw. Regulatory Perspective of Biomarker Bioanalysis During Drug Development.https://www.tandfonline.com/doi/full/10.4155/bio-2019-0029
- E. Rozet , R.D. Marini , E. Ziemons , B. Boulanger , Ph. Hubert. Advances in validation, risk and uncertainty assessment of bioanalytical methods.https://www.sciencedirect.com/science/article/abs/pii/S0731708510007235
- Stephen Keller, Jorge Quiroz ,Dave Christopher, Enaksha Wickremsinhe, Wanping Geng, Glen Hawthorne. The Effectiveness of Quality Control Samples in Pharmaceutical Bioanalysis.https://www.tandfonline.com/doi/abs/10.4155/bio-2020-0265

