Introduction: Why AET Derivation Is the Defining Step in E&L Studies
The Analytical Evaluation Threshold (AET) is the single most influential value in any extractables and leachables (E&L) study because it defines the entire scope of analytical investigation. If the AET is established too high, potentially harmful leachables may remain undetected and unreported. Conversely, if the threshold is set too low, laboratories may be forced to characterize large numbers of insignificant compounds, creating unnecessary analytical burden, increased timelines, and excessive study costs. For this reason, deriving the correct AET for Extractables and Leachables Studies is not simply an administrative exercise or an early-stage calculation. It is a scientifically critical decision that directly affects patient safety, regulatory compliance, toxicological assessment, and overall project efficiency.
At ResolveMass Laboratories Inc., we have consistently observed that many regulatory questions, deficiencies, and complete-response letters associated with E&L programs originate not from analytical instrumentation failures or extraction inefficiencies, but from poorly justified AET calculations. Regulatory agencies increasingly expect a transparent, scientifically supported rationale that explains exactly how the AET was established. This article explains the mechanistic reasoning, product-specific considerations, and population-based adjustments required to create an AET that is both scientifically robust and regulatorily defensible.
To understand how robust calculations form the foundation of compliant testing programs, explore our full suite of solutions at ResolveMass Extractables and Leachables Testing.
Share via:
Article Summary:
- The Analytical Evaluation Threshold (AET) is determined by working backward from the Safety Concern Threshold (SCT), while incorporating patient dosing parameters, administration route, and conservative exposure assumptions.
- Establishing a reliable AET requires product-specific considerations such as maximum daily dose, container usage frequency, target patient group (adult or pediatric), and the detection capability of the analytical method.
- Incorrect AET calculations can create significant regulatory concerns by either identifying too many insignificant compounds or failing to detect potentially harmful leachables that may affect patient safety.
- Regulatory frameworks including International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use Q3E, United States Pharmacopeia <1664.2>, and International Organization for Standardization 10993-17 apply different scientific approaches for AET derivation, making framework selection dependent on the product category and clinical application.
- This article explains the complete AET development workflow, including administration-route adjustments, container-closure system evaluation, pediatric exposure calculations, and conservative worst-case stacking methodologies.
- Common industry challenges — such as inaccurate surface-area normalization and unrealistic dosing assumptions — are also examined with practical scientific guidance for avoiding compliance issues.
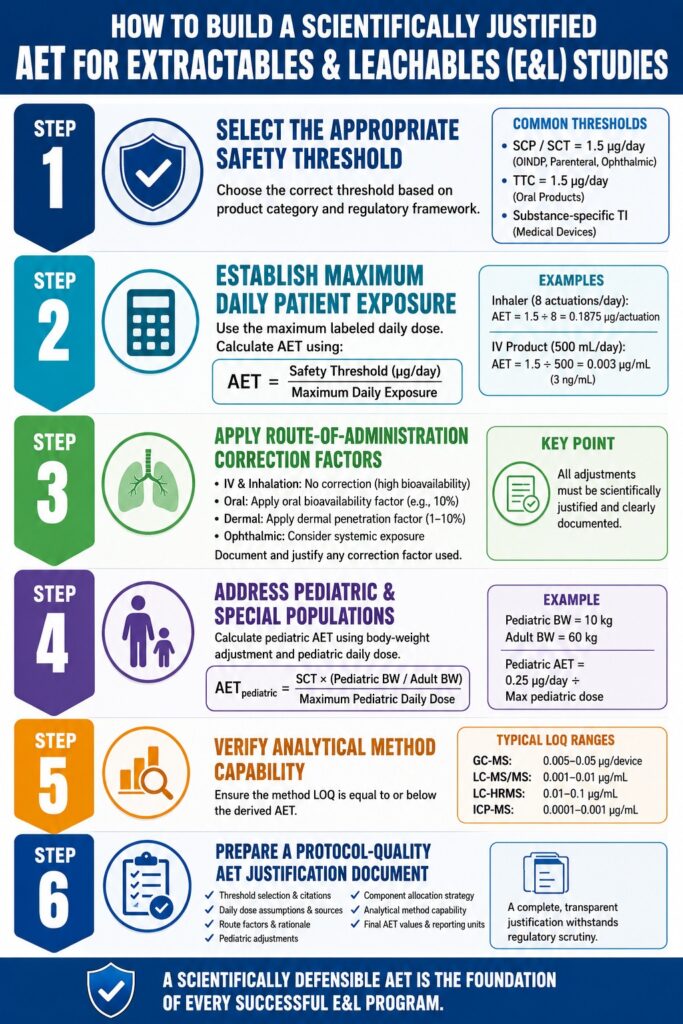
Step 1: Select the Appropriate Safety Threshold for the Product Category
The safety threshold selected as the starting point for the calculation fundamentally determines the final AET. If the incorrect threshold is used at the outset, every subsequent calculation becomes scientifically compromised.
| Product Category | Recommended Threshold Anchor | Regulatory Framework |
|---|---|---|
| Orally inhaled and nasal drug products (OINDP) | SCT = 1.5 μg/day | PQRI 2006, ICH Q3E |
| Parenteral and ophthalmic drug products | SCT = 1.5 μg/day (often more conservative in practice) | ICH Q3E, USP <1> |
| Oral solid and liquid dosage forms | TTC = 1.5 μg/day (adjusted using Cramer Class principles) | ICH M7, ICH Q3E |
| Medical devices with patient contact | Substance-specific Tolerable Intake (TI) | ISO 10993-17 |
| Combination products | Most conservative threshold from both frameworks | ICH Q3E + ISO 10993-17 |
A critical scientific distinction must be clearly understood here. The 1.5 μg/day value used for genotoxic impurities under ICH M7 is based on the Threshold of Toxicological Concern (TTC) concept for compounds with potential carcinogenic risk. By contrast, the 1.5 μg/day Safety Concern Threshold (SCT) used for OINDP products under PQRI guidance is derived from a different toxicological rationale focused on inhalation exposure risk. Although the numerical values are identical, the toxicological basis is different. These thresholds should never be treated as interchangeable without proper scientific justification.
Learn more about evolving global harmonization standards by reading our breakdown of the ICH Q3E Guideline for Extractables and Leachables.
Step 2: Establish the Maximum Daily Patient Exposure With Precision
The maximum daily patient exposure serves as the divisor in the AET equation. Any underestimation of patient exposure results in an artificially permissive AET, which can ultimately lead to under-reporting of clinically relevant leachables. Therefore, the calculation must always use the maximum labeled daily dose rather than the average, typical, or expected clinical dose.
For OINDP Products (Metered-Dose Inhalers, Dry Powder Inhalers, and Nasal Sprays)
The AET is commonly calculated using the following relationship:
AET (μg/device or μg/actuation)=SCT (μg/day)Maximum Daily ActuationsAET\,(\mu g/device\;or\;\mu g/actuation)=\frac{SCT\,(\mu g/day)}{Maximum\;Daily\;Actuations}AET(μg/deviceorμg/actuation)=MaximumDailyActuationsSCT(μg/day)
If an inhaler product is labeled for a maximum usage of 8 actuations per day:
AET=1.5 μg/day8 actuations=0.1875 μg/actuationAET=\frac{1.5\,\mu g/day}{8\,actuations}=0.1875\,\mu g/actuationAET=8actuations1.5μg/day=0.1875μg/actuation
This resulting AET is then applied on a per-actuation basis during extractables characterization of the device components.
For Parenteral Drug Products
The calculation is commonly expressed as:
AET (μg/mL or μg/container)=SCT (μg/day)Maximum Daily Volume (mL)AET\,(\mu g/mL\;or\;\mu g/container)=\frac{SCT\,(\mu g/day)}{Maximum\;Daily\;Volume\,(mL)}AET(μg/mLorμg/container)=MaximumDailyVolume(mL)SCT(μg/day)
For a parenteral product administered intravenously at a maximum daily volume of 500 mL:
AET=1.5 μg/day500 mL=0.003 μg/mL=3 ng/mLAET=\frac{1.5\,\mu g/day}{500\,mL}=0.003\,\mu g/mL=3\,ng/mLAET=500mL1.5μg/day=0.003μg/mL=3ng/mL
This calculation produces a highly stringent analytical target. Before finalizing the study design, the laboratory must confirm that the selected analytical methods possess sufficient sensitivity to achieve the required Limit of Detection (LOD) and Limit of Quantitation (LOQ).
Worst-Case Stacking Considerations
Modern drug delivery systems often contain multiple materials and container-closure components, including vials, stoppers, plungers, syringes, tubing, and connectors. When several components contribute simultaneously to patient exposure, the AET must either be distributed among those components or conservatively applied to each component independently under a worst-case assumption. Regulatory reviewers increasingly expect sponsors to explicitly describe and justify this stacking strategy within the study protocol and risk assessment documentation.
For a deeper look into standard protocols and testing expectations, see our comprehensive guide on ICH Q3E Extractables and Leachables E&L Study Requirements.
Step 3: Incorporate Route-of-Administration Correction Factors
The route of administration strongly influences systemic bioavailability, and systemic bioavailability directly affects toxicological exposure. Intravenous and inhalation products deliver compounds directly into systemic circulation, while orally administered products undergo first-pass metabolism and incomplete absorption. Consequently, route-specific adjustments are scientifically justified and frequently expected by regulatory authorities.
Intravenous and Inhalation Routes
For intravenous and inhalation products, no bioavailability correction factor is typically applied because these routes are considered high-bioavailability exposure pathways. The SCT is therefore used directly without modification.
Oral Products
In some oral product programs, sponsors apply an oral bioavailability adjustment factor. A common example is the assumption of 10% oral bioavailability, where the SCT is multiplied by 10 prior to division by the daily dose. This produces a less stringent AET. However, this approach is only scientifically acceptable when supported by adequate toxicological and pharmacokinetic justification for the relevant compound class.
Dermal and Transdermal Products
Dermal penetration corrections, commonly ranging from 1% to 10%, may be considered for dermal or transdermal products. Nevertheless, these adjustments require substance-specific penetration data to remain scientifically defensible during regulatory review.
Ophthalmic Products
Although ophthalmic drug products are administered in small volumes, systemic exposure through nasolacrimal drainage pathways must still be considered. At present, no universally accepted correction factor exists for ophthalmic administration, making conservative scientific justification especially important.
Documentation Expectations
Any bioavailability adjustment applied during AET derivation must be fully documented and scientifically supported. Regulatory agencies expect these assumptions to appear transparently within the study protocol and accompanying toxicological rationale. Silent spreadsheet adjustments without explanation are considered unacceptable from a regulatory perspective.
Discover how different dosage forms dictate testing frameworks in Extractables and Leachables in Pharmaceutical Products.
Step 4: Address Pediatric and Special Patient Populations
Pediatric populations often represent the most sensitive exposure group and therefore may determine the most conservative AET requirement. If a product label includes pediatric indications, the AET calculation must explicitly evaluate pediatric exposure scenarios.
A rigorous body-weight-adjusted calculation can be expressed as follows:
AETpediatric=SCT×(Pediatric Body WeightAdult Body Weight)Maximum Pediatric Daily DoseAET_{pediatric}=\frac{SCT\times\left(\frac{Pediatric\;Body\;Weight}{Adult\;Body\;Weight}\right)}{Maximum\;Pediatric\;Daily\;Dose}AETpediatric=MaximumPediatricDailyDoseSCT×(AdultBodyWeightPediatricBodyWeight)
Using a conservative pediatric body weight assumption of 10 kg compared with the standard 60 kg adult reference:
- Adult AET = 1.5 μg/day ÷ maximum adult dose
- Pediatric AET = 1.5 × (10/60) μg/day ÷ maximum pediatric dose = 0.25 μg/day ÷ maximum pediatric dose
The lower and more conservative AET value ultimately governs the study design.
Regulatory agencies such as the FDA and EMA pay particularly close attention to pediatric risk assessments in E&L programs. Failure to include pediatric considerations when the product labeling supports pediatric use is a common and significant regulatory deficiency.
To ensure your program accounts for all vulnerable demographics, reference our guide on ICH Q3E Extractables Leachables E&L Risk Assessment.
Step 5: Verify Analytical Method Capability Relative to the Derived AET
An AET has practical value only if the analytical methodology can reliably detect and quantify compounds at or below that threshold. Therefore, analytical sensitivity must be confirmed before the study design is finalized.
| Analytical Technique | Typical LOQ Range | Suitable for AET ≥ |
|---|---|---|
| GC-MS (headspace or thermal desorption) | 0.005–0.05 μg/device | ~0.01 μg/device |
| LC-MS/MS (targeted analysis) | 0.001–0.01 μg/mL | ~0.005 μg/mL |
| LC-HRMS (non-targeted analysis) | 0.01–0.1 μg/mL | ~0.05 μg/mL |
| ICP-MS (elemental impurities) | 0.0001–0.001 μg/mL | ~0.001 μg/mL |
| Ion Chromatography | 0.01–0.1 μg/mL | ~0.05 μg/mL |
If the calculated AET falls below the achievable LOQ of the selected analytical platform, several scientifically acceptable approaches may be considered:
- Improve analytical sensitivity by optimizing extraction efficiency, increasing injection volume, or using more selective detection techniques.
- Apply a scientifically justified bioavailability correction that permits a less stringent AET.
- Implement concentration strategies or tiered extraction approaches to enrich analytes prior to analysis.
Whichever strategy is selected, the rationale must be clearly documented in the study protocol. Regulatory reviewers expect to see explicit evidence that method capability was evaluated against the calculated AET before study initiation.
Ensure your laboratory methodologies line up with baseline criteria by reviewing USP Extractables and Leachables.
Step 6: Prepare a Protocol-Quality AET Justification Document
The AET derivation package should function as a stand-alone scientific justification capable of withstanding detailed regulatory scrutiny. It should clearly and comprehensively include:
- The selected safety threshold, including SCT, TTC, or substance-specific Tolerable Intake values, together with supporting regulatory or literature citations
- The maximum daily dose assumption and its source, such as product labeling, prescribing information, or worst-case clinical usage scenarios
- Any applied route-of-administration or bioavailability correction factors, accompanied by scientific rationale
- Pediatric or special-population adjustments where applicable
- Component-specific allocation strategies for multi-component systems
- Verification that the selected analytical methods can achieve the derived AET
- The final AET values expressed in the appropriate reporting units, including μg/actuation, μg/device, μg/mL, or ng/mL
This justification should never be treated as a minor appendix table. Regulatory authorities frequently review AET documentation line by line because it forms the scientific foundation of the entire E&L program.
For detailed documentation formatting for submissions, view our outline on Extractables and Leachables E&L Requirements for U.S. Market Authorization.
Common AET Derivation Errors and Strategies to Prevent Them
| Error | Consequence | Correct Scientific Approach |
|---|---|---|
| Using average dose instead of maximum labeled dose | Produces an overly permissive AET and increases under-reporting risk | Always use the maximum labeled daily dose |
| Ignoring multi-component exposure stacking | Makes individual component AETs artificially lenient | Apply conservative worst-case stacking or allocate across all components |
| Applying oral bioavailability corrections without justification | Creates regulatory concern and may trigger study repetition | Support all correction factors with literature and scientific rationale |
| Omitting pediatric AET calculations for pediatric products | Results in major regulatory deficiencies | Calculate pediatric AET whenever pediatric labeling exists |
| Selecting an AET below the method LOQ without mitigation | Leads to unreliable analytical conclusions | Confirm analytical capability before study execution |
| Reporting AET values in incorrect units | Causes interpretation and comparison errors | Match reporting units precisely to extraction and analytical methodology |
Explore practical lessons learned from real filings in FDA Extractables and Leachables Case Studies.
Conclusion: A Scientifically Defensible AET Is the Core of Every E&L Program
A scientifically justified AET for Extractables and Leachables Studies is not merely a mathematical value calculated once and archived. It is an integrated scientific rationale that links clinical exposure, patient vulnerability, toxicological risk, and analytical capability into one defensible framework. Every downstream decision in an E&L program — including compound identification, toxicological qualification, reporting thresholds, and regulatory submissions — ultimately depends on the integrity of this calculation.
At ResolveMass Laboratories Inc., our E&L study strategies begin with a detailed and scientifically rigorous AET derivation process tailored to the specific product configuration, route of administration, patient population, and applicable regulatory framework. Investing in robust scientific justification at the beginning of the study significantly reduces the risk of regulatory deficiencies, repeat studies, delayed approvals, and costly remediation activities later in development.
Ready to secure your regulatory pathway? Learn what to look for when choosing an analytical partner in our article, Outsourcing Extractables and Leachables E&L Testing Laboratory United States.
Frequently Asked Questions About AET for Extractables and Leachables Studies
For orally inhaled and nasal drug products (OINDP), the commonly accepted Safety Concern Threshold (SCT) is 1.5 μg/day, as recommended by the PQRI framework. This threshold represents an exposure level at which a leachable compound is considered to present minimal toxicological concern under normal use conditions. It serves as the foundation for calculating the Analytical Evaluation Threshold (AET) in inhalation and nasal drug product studies. Regulatory agencies generally expect this value to be used unless a product-specific toxicological assessment justifies a different approach.
Using a single AET across all components in a multi-component system is generally not scientifically appropriate. Components such as stoppers, plungers, syringes, tubing, and vials can all contribute independently to the total patient exposure. Therefore, the cumulative leachable burden from all product-contact materials must remain within the permitted safety threshold. In most cases, the AET is either assigned individually to each component under a worst-case scenario or apportioned across the entire system with proper scientific justification.
Extractables studies and leachables studies serve different scientific purposes, which affects how the AET is applied. In extractables studies, exaggerated extraction conditions are used to identify compounds that could potentially migrate from packaging or device materials. The AET in these studies is commonly expressed relative to extraction solvent volume. In leachables studies, however, the threshold is tied directly to actual patient exposure conditions, meaning the AET is usually expressed per dose, per container, or per milliliter. Because leachables studies reflect real product usage, the associated AET is often more stringent.
A bioavailability correction factor is not mandatory for oral drug products, but it may be scientifically acceptable when supported by appropriate data and justification. Some sponsors apply a ten-fold adjustment based on the assumption of approximately 10% oral bioavailability, which can produce a less restrictive AET. However, regulatory acceptance of this approach depends heavily on the quality of the scientific rationale and supporting literature. For inhalation and parenteral products, bioavailability corrections are typically not applied because systemic exposure is assumed to be high.
When a product is intended for pediatric use, the AET calculation must specifically account for pediatric exposure scenarios. This is typically done by adjusting the calculation using pediatric body weight and maximum pediatric daily dose values. In many cases, the pediatric AET becomes more conservative than the adult value because children have lower body weight but may still receive significant exposure relative to size. Regulatory authorities expect these calculations to be clearly documented, especially for products with labeled pediatric indications.
If the derived AET falls below the Limit of Quantitation (LOQ) achievable by the analytical method, the issue must be addressed before study execution. One option is to improve analytical sensitivity by optimizing extraction techniques, increasing sample concentration, or selecting more sensitive instrumentation. Another approach involves applying a scientifically justified correction factor that relaxes the threshold appropriately. Concentration or enrichment strategies may also be used to improve detectability. Regulatory agencies generally consider it unacceptable to proceed with a study if the method cannot reliably achieve the required AET.
ICH Q3E builds upon many principles originally introduced through the PQRI framework but expands the guidance to cover a broader range of pharmaceutical products and delivery systems. The core toxicological concepts remain largely aligned, including the use of threshold-based safety principles. However, ICH Q3E provides more structured expectations for route-specific exposure assessment, multi-component systems, and risk-based justification strategies. For modern submissions, sponsors are increasingly expected to align their AET derivation approaches with ICH Q3E while still recognizing earlier PQRI-based methodologies where appropriate.
For a unit-dose nebulizer ampoule, the AET calculation is based on the number of ampoules a patient may use in a single day combined with the volume contained in each ampoule. In contrast, for a multi-dose vial, the AET is calculated using the total maximum daily administered volume from the vial. The key scientific distinction lies in how daily exposure is distributed across individual containers or repeated uses. Because patient exposure patterns differ between these dosage formats, the calculation strategy must accurately reflect real clinical usage.
Reference:
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. (2025). ICH harmonised guideline: Guideline for extractables and leachables Q3E (Draft version, Step 2). ICH Database PDF
- United States Pharmacopeia. (2020). 〈1663〉 Assessment of extractables associated with pharmaceutical packaging/delivery systems. In USP–NF. United States Pharmacopeial Convention. https://doi.org/10.31003/USPNF_M7126_03_01
- United States Pharmacopeia. (2016, July 29). 〈1664〉 Assessment of drug product leachables associated with pharmaceutical packaging/delivery systems—Errata. USP–NF. https://www.uspnf.com/errata/assessment-drug-product-leachables-associated-pharmaceutical-packagingdelivery-systems-2016
- International Organization for Standardization. (2020). ISO 10993-18:2020 biological evaluation of medical devices—Part 18: Chemical characterization of medical device materials within a risk management process. https://www.iso.org/standard/64750.html
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. (2023). ICH harmonised guideline: Assessment and control of DNA reactive (mutagenic) impurities in pharmaceuticals to limit potential carcinogenic risk M7(R2). https://database.ich.org/sites/default/files/ICH_M7(R2)_Guideline_Step4_2023_0216_0.pdf

