Introduction
Sustained-release ocular drug delivery continues to represent a major bioengineering challenge because the eye possesses multiple anatomical and physiological defense mechanisms designed to prevent the entry of foreign substances. Conventional topical ophthalmic formulations, particularly eye drops, demonstrate extremely poor ocular bioavailability, commonly ranging between less than 1% and 5%. This limited absorption occurs because of continuous tear turnover, reflex blinking, and rapid nasolacrimal drainage, all of which quickly eliminate the administered drug from the ocular surface.
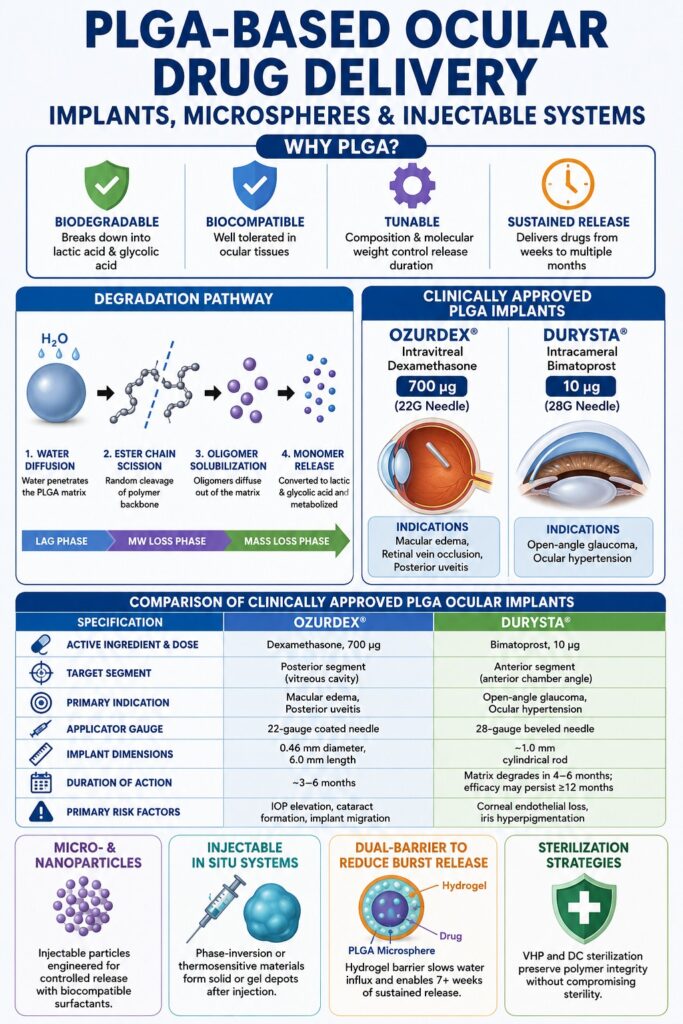
To overcome these physiological barriers, modern ophthalmic practice frequently utilizes direct intravitreal or intracameral injections. Although these approaches significantly improve drug delivery to intraocular tissues, repeated injections are associated with substantial clinical risks, including endophthalmitis, retinal detachment, subconjunctival hemorrhage, and poor long-term patient compliance. These limitations have accelerated the development of PLGA-Based Ocular Drug Delivery systems, which provide biodegradable, biocompatible, and highly tunable platforms capable of delivering therapeutic agents directly to targeted ocular tissues for extended durations ranging from several weeks to multiple months.
Explore Comprehensive Formulation Options: To learn how PLGA-based matrices are engineered for long-term therapeutic delivery across various administration routes, visit our technical guide on PLGA long-acting injectable formulations.
Executive Summary:
- PLGA-based ocular drug delivery systems are being developed to overcome the poor bioavailability of conventional eye drops, which are rapidly cleared from the eye by blinking, tear turnover, and nasolacrimal drainage.
- These biodegradable polymer platforms enable sustained and targeted drug release inside the eye for weeks or months, reducing the need for repeated intravitreal or intracameral injections and improving patient compliance.
- The degradation behavior of PLGA depends on factors such as lactide-to-glycolide ratio, molecular weight, and end-group chemistry, all of which influence water penetration, erosion rate, and drug release duration.
- Clinically approved PLGA implants such as Ozurdex and Durysta provide long-acting treatment for retinal diseases, macular edema, glaucoma, and ocular hypertension through controlled intraocular drug delivery.
- Ozurdex delivers dexamethasone into the vitreous cavity for posterior eye disorders, while Durysta releases bimatoprost into the anterior chamber to reduce intraocular pressure in glaucoma patients.
- Advanced PLGA microspheres and nanoparticles offer minimally invasive injectable delivery options, but their safety and effectiveness depend heavily on particle size, surface properties, and surfactant selection.
- Injectable phase-inversion systems and thermosensitive hydrogels can transform from liquids into solid or gel depots after administration, enabling prolonged therapeutic release with less invasive procedures.
- Future advancements in PLGA ocular delivery are expected to include multifunctional systems such as drug-eluting contact lenses, bioadhesive nanoparticles, and smart implant technologies designed for precise and long-term ocular therapy.
Mechanisms of Polymer Degradation in PLGA-Based Ocular Drug Delivery
PLGA degradation within the intraocular environment occurs primarily through random hydrolytic cleavage of the polymer’s ester backbone. This degradation process gradually converts the polymer into non-toxic lactic acid and glycolic acid monomers, which are subsequently metabolized and eliminated through normal physiological pathways. The degradation kinetics of PLGA can be precisely engineered by modifying the lactide-to-glycolide monomer ratio, altering the weight-average molecular weight (Mw), and selecting appropriate polymer end-group capping strategies that regulate water penetration and bulk erosion behavior.
[H2O] Diffusion
PLGA ───────────────────> Random Ester Chain Scission ───> Oligomer Solubilization ───> Bulk Erosion & Monomer Release
(Phase 1: Lag Phase) (Phase 2: Molecular Weight Loss) (Phase 3: Mass Loss & Acid Release)The hydrophobicity of the copolymer components strongly influences the overall degradation profile. Lactic acid contains a hydrophobic methyl side group that restricts water penetration into the polymer matrix, whereas glycolic acid lacks this side chain and therefore exhibits substantially greater hydrophilicity. As a result, PLGA copolymers enriched with lactide absorb less water and degrade more slowly.
Among commonly used formulations, the 50:50 lactide ratio exhibits the most rapid degradation profile, generally degrading within approximately 30 to 40 days because of its highly amorphous structure and elevated water-swelling capacity. Increasing the lactide proportion to ratios such as 75:25 or 85:15 substantially slows degradation kinetics, making these compositions particularly suitable for long-acting posterior segment implants intended to deliver drugs over periods extending from 3 to 6 months.
Polymer end-group chemistry also plays a critical role in degradation behavior. Acid-terminated (uncapped) PLGA contains free terminal carboxylic acid groups that readily hydrate and lower the internal matrix pH. This acidic microenvironment promotes autocatalytic bulk hydrolysis, thereby accelerating polymer degradation. In contrast, ester-terminated PLGA, which is capped with alkyl esters such as methyl or lauryl groups, reduces water uptake and minimizes premature acidification within the matrix, resulting in slower and more controlled polymer erosion.
Compare Biomaterial Erosion Mechanisms: For an in-depth mechanical breakdown of how matrix composition dictates water uptake and structural degradation, view our analysis of bulk erosion vs surface erosion in PLGA.
Influence of Polymer Characteristics on PLGA Degradation and Release Profiles
| Polymer Parameter | Physical Mechanism | Impact on Degradation Rate | Impact on Ocular Suitability |
|---|---|---|---|
| High Lactide Content (e.g., 75:25, 85:15) | Hydrophobic methyl side groups reduce water penetration into the polymer matrix. | Significantly decreased | Suitable for long-acting posterior segment implants providing 3–6 months of delivery. |
| Equimolar Monomer Ratio (50:50 L) | Maximizes amorphous polymer regions and water absorption capacity. | Extremely increased | Appropriate for short-term therapeutic delivery and rapid-release injectable systems. |
| High Molecular Weight (Mw > 50,\text{kDa}) | Long polymer chains require extensive ester cleavage before mass loss occurs. | Decreased | Extends structural integrity of intravitreal rods and minimizes premature fragmentation. |
| Acid-Terminated End-Groups | Free carboxylic acid groups decrease internal matrix pH and induce autocatalytic cleavage. | Significantly increased | Useful for biphasic release profiles but may increase the risk of local tissue irritation. |
| Ester-Terminated Capping | Non-reactive alkyl-capped end groups minimize hydration and internal acidification. | Decreased | Reduces initial burst release and improves long-term formulation stability. |
Analyze Controlled Kinetic Modalities: To see how specific monomer selections modulate real-world therapeutic release rates, check out our report on PLGA ratio release kinetics.
Clinically Approved Sustained-Release Implants
Clinically approved PLGA-based ocular implants, including Ozurdex and Durysta, provide prolonged therapeutic efficacy by continuously releasing active pharmaceutical ingredients directly into targeted ocular compartments while simultaneously undergoing complete in vivo biodegradation. These advanced systems utilize specially engineered preloaded applicators designed to ensure accurate placement within either the vitreous cavity or anterior chamber.
┌──────────────────────────────────────────────┐
│ CLINICALLY APPROVED PLGA SUSTAINED-RELEASE │
│ IMPLANTS │
└──────┬────────────────────────────────┬──────┘
│ │
┌──────────────▼──────────────┐ ┌──────────────▼──────────────┐
│ OZURDEX │ │ DURYSTA │
│ Intravitreal Dexamethasone│ │ Intracameral Bimatoprost │
│ 700 µg (22G Needle) │ │ 10 µg (28G Needle) │
└──────────────┬──────────────┘ └──────────────┬──────────────┘
│ │
┌──────────────▼──────────────┐ ┌──────────────▼──────────────┐
│ Retinal Vein Occlusion / DME│ │ Open-Angle Glaucoma / │
│ Posterior Segment Uveitis │ │ Ocular Hypertension │
└─────────────────────────────┘ └─────────────────────────────┘Optimize Depot Engineering Protocols: For technical insights into designing solid rod and cylinder delivery matrices, read our deep-dive into PLGA depot formulations.
Clinical Applications of PLGA-Based Ocular Drug Delivery via Ozurdex
Ozurdex is a biodegradable intravitreal implant containing 700 micrograms of dexamethasone embedded within a PLGA matrix and is designed to treat retinal vascular disorders and posterior uveitis. Administration is performed using a specialized 22-gauge applicator needle that forms a self-sealing scleral tunnel during implantation.
Ozurdex is indicated for macular edema secondary to branch retinal vein occlusion (BRVO) or central retinal vein occlusion (CRVO), diabetic macular edema (DME) in pseudophakic patients, and non-infectious posterior segment uveitis. The implant itself is rod-shaped, measuring approximately 0.46 mm in diameter and 6 mm in length. It is preloaded into a customized single-use applicator equipped with a glide-enhancing coated 22-gauge needle that facilitates smooth scleral penetration and controlled implantation.
The injection is performed through the pars plana using a tunneled scleral pathway to minimize vitreous leakage and prevent wound gaping. Clinical studies have demonstrated that the dexamethasone-containing PLGA matrix gradually dissolves over several months while continuously releasing corticosteroid therapy.
However, corticosteroid administration is associated with well-recognized class-specific adverse effects. Elevation of intraocular pressure (IOP) typically peaks around week 8 following implantation, requiring pharmacological treatment in approximately 25% of patients and surgical intervention in roughly 1% of cases. Posterior subcapsular cataract formation has been reported in up to 68% of patients receiving repeated multi-year injections for DME management.
Following implantation, patients require careful post-procedural monitoring using tonometry and slit-lamp biomicroscopy to detect complications such as endophthalmitis, retinal detachment, or anterior chamber implant migration, particularly in eyes with compromised posterior lens capsules.
Clinical Applications of PLGA-Based Ocular Drug Delivery via Durysta
Durysta represents the first biodegradable intracameral implant containing 10 micrograms of bimatoprost specifically engineered to reduce intraocular pressure in patients diagnosed with open-angle glaucoma or ocular hypertension. The implant is administered directly into the anterior chamber using a preloaded 28-gauge needle applicator.
Durysta directly targets both the trabecular meshwork pathway and the uveoscleral outflow pathway. The implant consists of a cylindrical rod approximately 1 mm in length composed of multiple PLGA polymer grades, including poly(D,L-lactide), poly(D,L-lactide-co-glycolide), and polyethylene glycol (PEG) 3350, which functions as a plasticizing excipient.
During the outpatient procedure, the preloaded applicator enters the anterior chamber through a small clear corneal incision and releases the implant into the aqueous environment. Patients are instructed to remain upright for at least one hour after implantation to ensure gravitational settling of the implant into the inferior iridocorneal angle at the 6 o’clock position.
Phase 3 ARTEMIS clinical trials demonstrated that a single Durysta implant achieved non-inferiority compared with twice-daily topical timolol 0.5%, producing approximately 30% reductions in IOP corresponding to decreases of 5–8 mmHg. Interestingly, although the PLGA matrix physically degrades within approximately 4 to 6 months, therapeutic IOP reduction may persist for 12 to 24 months in a considerable proportion of patients.
This prolonged pharmacological activity is believed to result from bimatoprost-induced tissue remodeling within the trabecular meshwork and ciliary body. Despite its effectiveness, repeated implantation remains limited because of concerns regarding corneal endothelial cell density loss. Consequently, gonioscopy is required before implantation to confirm an adequately open iridocorneal angle (Shaffer grade \ge 3) together with sufficient endothelial cell reserves.
Permanent iris hyperpigmentation has been documented in approximately 1% to 5% of treated patients.
Comparative Specifications of Clinically Approved PLGA Ocular Implants
| Specification Parameter | Ozurdex Intravitreal Implant | Durysta Intracameral Implant |
| Active Ingredient & Dose | Dexamethasone, 700 µg | Bimatoprost, 10 µg |
| Target Ocular Segment | Posterior segment (vitreous cavity) | Anterior segment (anterior chamber angle) |
| Anatomical Target | Retina, macula, choroid | Trabecular meshwork, ciliary body |
| Excipient Composition | Biodegradable PLGA matrix | Poly(D,L-lactide), poly(D,L-lactide) acid-end, poly(D,L-lactide-co-glycolide), PEG 3350 |
| Applicator Device Gauge | 22-gauge coated needle | 28-gauge beveled needle |
| Implant Dimensions | 0.46 mm diameter, 6.0 mm length | Approximately 1.0 mm cylindrical rod |
| Primary Clinical Indication | Macular edema and posterior segment uveitis | Open-angle glaucoma and ocular hypertension |
| Clinical Persistence Duration | Approximately 3–6 months | Matrix degrades in 4–6 months; efficacy may persist \ge 12 months |
| Primary Risk Factors | IOP elevation, cataract formation, implant migration | Corneal endothelial loss, iris hyperpigmentation |
Evaluate Alternative Sustained-Release Polymers: To compare the performance of PLGA against other gold-standard biodegradable options, review our side-by-side PLA vs PLGA vs PCL evaluation.
Advanced Micro- and Nanoparticulate Systems
PLGA microspheres and nanoparticles are advanced particulate delivery systems that provide the significant advantage of injectability through fine-gauge needles without requiring large mechanical implantation devices. However, the successful formulation of these systems requires strict control of particle size distribution, surface charge characteristics, and surfactant-related toxicity to prevent undesirable biological reactions.
Double-Emulsion Fabrication and Surfactant Optimization
PLGA micro- and nanoparticles are commonly synthesized using a water-in-oil-in-water (W1/O/W2) double-emulsion solvent extraction/evaporation process designed specifically for encapsulating hydrophilic active pharmaceutical ingredients. The selection of surfactants such as polyvinyl alcohol (PVA) or Pluronic F-108 is essential for maintaining colloidal stability while minimizing cellular toxicity.
The fabrication process begins with dissolution of the active therapeutic compound within an aqueous internal phase (W1). This aqueous phase is subsequently emulsified into an organic solvent phase containing dissolved PLGA polymer, typically dichloromethane (O). High-shear homogenization or ultrasonication is then applied to generate a fine primary W1/O emulsion.
The resulting primary emulsion is transferred into a secondary aqueous phase (W2) containing a stabilizing surfactant such as PVA and emulsified again to generate the final W1/O/W2 double emulsion. To solidify the droplets into hardened microspheres, the organic solvent is extracted using an aqueous extraction medium, commonly containing 2% isopropanol, followed by sieving, washing, freezing, and lyophilization.
Step 1: Primary Emulsion (W1/O)
┌──────────────────────────┐ Ultrasonication
│ Aqueous API (W1) ├────────────────────────>
│ + PLGA in DCM Solvent (O)│
└──────────────────────────┘
Step 2: Double Emulsion (W1/O/W2)
┌──────────────────────────┐ Ultrasonication
│ Primary Emulsion (W1/O) ├────────────────────────>
│ + Aqueous Surfactant (W2)│
└──────────────────────────┘
Step 3: Hardening and Isolation
┌──────────────────────────┐ Solvent Extraction
│ Double Emulsion ├────────────────────────> [ Hardened Microspheres ] ───> Sieving & Lyophilization
│ + Isopropanol/Water │
└──────────────────────────┘The surfactant selected for the W2 phase significantly influences particle size, entrapment efficiency, and biological compatibility. Polyvinyl alcohol remains the standard stabilizer because it consistently produces uniform particles with high drug encapsulation efficiency. Pluronic F-108 is also considered highly biocompatible and produces nanoparticles averaging approximately 113.4,\text{nm} with minimal cytotoxicity.
Chitosan coatings may be applied to generate positively charged particles exhibiting zeta potentials near +31.0,\text{mV}, thereby improving mucoadhesion and corneal penetration. However, ocular toxicity studies indicate that chitosan concentrations between 200 and 500,\mu\text{g/mL} can induce substantial cellular toxicity after 48 hours of exposure. In contrast, PVA and Pluronic F-108 maintain favorable cytocompatibility profiles without triggering significant inflammatory responses.
Master Particulate Release Dynamics: To learn how structural polymer properties influence diffusion kinetics specifically in micro-scale delivery vehicles, read about PLGA for controlled release systems.
Ocular Tolerability and Particulate Size-Exclusion Thresholds
Intravitreal injection of PLGA microspheres measuring between 20 and 100 micrometers can provoke severe chronic foreign body reactions, whereas solid rod-shaped implants containing equivalent polymer masses are generally well tolerated. This critical observation demonstrates that particulate systems with high surface-area-to-volume ratios strongly promote macrophage activation and inflammatory cytokine release.
Preclinical investigations in rabbits and non-human primates revealed profound immunological differences among various PLGA dosage forms. Intravitreal administration of 3,\text{mg} to 12.5,\text{mg} of free PLGA microspheres measuring 20 to 100,\mu\text{m} in diameter produced severe ocular immune responses characterized by vitritis, vitreous haze, and chronic foreign body inflammation.
Histological examination demonstrated active macrophage clustering and phagocytosis surrounding the microparticles, resulting in elevated secretion of pro-inflammatory mediators including tumor necrosis factor-alpha (TNF-\alpha) and interleukin-6 (IL-6).
Conversely, implantation of monolithic PLGA rods containing equivalent polymer masses, such as Ozurdex-type systems, did not trigger detectable inflammatory or immune reactions within the vitreous cavity. In vitro studies using peripheral blood mononuclear cells (PBMCs) and isolated macrophages further confirmed that particulate PLGA formulations stimulate cytokine release, whereas monolithic implants remain largely immunologically inert.
These findings demonstrate that geometry, total exposed surface area, and particle topography are critical quality attributes (CQAs) governing ocular biocompatibility. Consequently, particulate ocular delivery systems require highly controlled size-exclusion filtration and advanced surface-modification strategies to minimize immune recognition by ocular macrophages.
Injectable Phase-Inversion and Thermosensitive Systems
Injectable PLGA formulations can be engineered to undergo in situ phase inversion or temperature-responsive sol-to-gel transitions, allowing them to transform from syringeable liquids into solid therapeutic depots after administration into physiological environments. These systems combine the convenience of minimally invasive liquid injection with the prolonged release characteristics of solid implants.
Phase-Inversion In Situ Implants
Phase-inversion systems are prepared by dissolving PLGA copolymers, such as 50:50 or 75:25 formulations, within water-miscible organic solvents such as N-methyl-2-pyrrolidone (NMP) together with the active pharmaceutical ingredient. Following injection into aqueous ocular tissues, the solvent rapidly diffuses outward into surrounding physiological fluids, causing polymer precipitation and formation of a solid implant matrix.
These formulations exhibit pseudoplastic shear-thinning rheological behavior, meaning they maintain low viscosity under high shear stress conditions, thereby allowing smooth injection through fine-gauge needles. After injection into aqueous environments such as the vitreous humor, rapid solvent exchange occurs. NMP diffuses outward while water diffuses inward into the hydrophobic PLGA phase, creating thermodynamic instability that induces polymer precipitation and solid implant formation.
Optical coherence tomography (OCT) studies have confirmed that phase-inversion implants solidify rapidly after injection, with matrix thickness stabilizing as the system transitions into a durable drug depot capable of sustained release over several weeks.
Thermosensitive Hydrogels
Thermosensitive systems are based on triblock copolymers such as PLGA-PEG-PLGA that exhibit temperature-dependent sol-to-gel transitions near physiological temperature. These materials remain in a liquid state at room temperature, enabling convenient topical administration or injection, but rapidly transform into viscous hydrogel depots when exposed to ocular temperatures.
PLGA-PEG-PLGA triblock copolymers are synthesized through ring-opening polymerization of lactide and glycolide monomers using PEG as an initiator molecule. The amphiphilic polymer self-assembles into micellar structures in cold aqueous environments, generating a free-flowing injectable solution.
Upon exposure to ocular temperatures ranging from 35^\circ\text{C} to 37^\circ\text{C}, dehydration of PEG chains occurs together with enhanced hydrophobic interactions among PLGA segments. These interactions induce micellar aggregation and hydrogel network formation.
This property is especially advantageous for anterior segment topical drug delivery. Incorporating PLGA nanoparticles loaded with anti-inflammatory corticosteroids such as hydrocortisone butyrate into thermosensitive PLGA-PEG-PLGA hydrogel matrices markedly prolongs precorneal residence time, minimizes rapid nasolacrimal washout, and enables sustained corneal absorption without substantial systemic exposure.
Strategies to Mitigate the Initial Burst Release
Initial burst release refers to the rapid and uncontrolled liberation of a substantial fraction of encapsulated drug during the first hours following administration. This phenomenon primarily results from surface-associated drug molecules together with rapid water penetration into the polymer matrix and may lead to localized toxicity.
The underlying mechanism of burst release is closely associated with thermodynamic drug migration during fabrication. During solvent extraction and microsphere solidification, water-soluble drugs tend to partition toward the external aqueous phase and become concentrated near the microsphere surface. Following clinical administration, these surface-bound molecules dissolve immediately.
Simultaneously, rapid water influx into the porous PLGA matrix accelerates swelling and creates open diffusion channels that permit premature drug escape before hydrolytic erosion begins.
To reduce this effect, formulation scientists frequently employ dual-barrier delivery approaches in which drug-loaded PLGA microspheres are embedded within secondary hydrogel matrices. A representative example involves the development of drug-eluting intraocular lenses (IOLs) designed for postoperative cataract management.
In these systems, timolol maleate is first encapsulated within PLGA microspheres using a W/O/W double-emulsion method. The microspheres are subsequently incorporated into poly(acrylamide-sodium acrylate) hydrogel (PAH) films forming the non-optical haptic region of the IOL.
Dual-Barrier Controlled Release:
┌───────────────────────────────┐
│ Aqueous Medium (Eye) │
└──────────────┬────────────────┘
│ Water Diffusion
▼
=============================
* * * * * * *
=============================
│ Slowing Hydrolysis
▼
┌─────────────────────────────┐
│ Timolol API sustained over │
│ 7+ Weeks │
└─────────────────────────────┘The external hydrogel barrier slows water penetration into the embedded PLGA microspheres, thereby delaying polymer swelling and hydrolysis. This dual-system architecture enables continuous timolol release for periods exceeding 7 weeks while substantially reducing the magnitude of the initial burst release.
Importantly, embedding PLGA microspheres within the PAH matrix slows polymer degradation sufficiently to produce approximately three-fold increases in therapeutic duration compared with standalone microsphere formulations.
Assess Monodispersity and Stability Dynamics: To analyze how maintaining a narrow polydispersity index controls structural uniformity and prevents burst release spikes, consult our report on pharmaceutical PLGA PDI parameters.
Sterilization Challenges and Material Integrity
Sterilization of PLGA-based ocular systems presents considerable technical challenges because many conventional industrial sterilization methods, including autoclaving, gamma irradiation, and ethylene oxide exposure, can damage the polymer backbone, alter physical morphology, or leave toxic residual contaminants.
Maintaining sterility while preserving critical quality attributes such as molecular weight, glass transition temperature, mechanical integrity, and release kinetics requires highly specialized sterilization approaches.
Gamma and Electron-Beam (E-Beam) Radiation
Ionizing radiation transfers substantial energy into PLGA polymers, inducing homolytic cleavage of ester bonds within PLA, PGA, and PLGA chains. Radiation scission yields (Gs) substantially exceed cross-linking yields (Gx), producing rapid decreases in weight-average molecular weight (Mw) and reductions in glass transition temperature (Tg).
These alterations accelerate in vivo degradation and may trigger premature implant erosion accompanied by localized acidic microenvironments caused by accelerated monomer release.
Ethylene Oxide (EO)
Although EO sterilization is effective at relatively low temperatures, its application to PLGA systems is complicated by toxic residual chemicals and mechanical deformation effects. EO gas acts as a plasticizer that can cause swelling, shrinkage, or deformation of PLGA structures. Studies have demonstrated that porous PLGA scaffolds may shrink by as much as 60% of their original volume during EO sterilization cycles.
Vaporized Hydrogen Peroxide (VHP)
VHP sterilization provides a milder alternative that sterilizes device surfaces using hydrogen peroxide vapor without substantially penetrating or degrading the polymer bulk. PLGA scaffolds sterilized using VHP maintain smooth surface morphology, structural porosity, and mechanical integrity without significant shrinkage.
Direct-Current (DC) Sterilization
An emerging sterilization strategy involves low-voltage direct-current electrical treatment. Applying direct current voltages of 4–6 V across electrospun PLGA scaffolds for approximately 30–40 seconds has demonstrated complete bactericidal efficacy without detectable alterations in polymer molecular weight or fiber morphology. This approach represents a promising sterilization method for highly sensitive biodegradable ocular systems.
Analytical Validation and Regulatory Sameness Workflows
Demonstrating the quality, safety, and regulatory equivalence of PLGA-based ocular systems requires comprehensive multi-tiered analytical characterization capable of defining polymer molecular weight distribution, monomer composition, thermal behavior, and impurity profiles.
Specialized CDMOs such as ResolveMass Laboratories Inc. provide advanced instrumentation and validated analytical methodologies necessary for compliance with international regulatory standards governing complex drug-device combination products.
Q1/Q2 Polymer Equivalence and Characterization
To ensure predictable and reproducible in vivo performance, analytical workflows must comprehensively characterize PLGA degradation behavior throughout all hydrolytic stages. This characterization relies on integrated applications of size-exclusion chromatography, nuclear magnetic resonance spectroscopy, and thermal analysis techniques.
Gel Permeation Chromatography (GPC) coupled with multi-angle light scattering (MALS) serves as the primary analytical technique for determining molecular weight distribution, number-average molecular weight (Mn), weight-average molecular weight (Mw), and polydispersity index (PDI).
Execute Advanced Molecular Weight Assays: For validated protocols on evaluating molecular weight and PDI using absolute light scattering techniques, view our breakdown of PLGA polymer molecular weight and PDI.
Quantitative Nuclear Magnetic Resonance (qNMR) spectroscopy is utilized to verify precise lactide-to-glycolide ratios through integration of lactide methyl proton signals near \sim 1.5,\text{ppm} relative to glycolide methylene proton signals near \sim 4.8,\text{ppm}.
Verify Precise Copolymer Composition: To review ultra-high-resolution methodologies for determining exact molar ratios, see our methodology for NMR spectroscopy for accurate monomer ratios.
Differential Scanning Calorimetry (DSC) is employed to determine glass transition temperature (Tg) and polymer crystallinity, both of which strongly influence mechanical properties and water permeability. Thermogravimetric Analysis (TGA) is commonly performed concurrently to evaluate moisture content and thermal decomposition behavior.
Establish Structural Sameness Frameworks: For a step-by-step review of complete analytical workflows mapping out regulatory equivalence, explore our specialized approach to Q1/Q2 polymer equivalence assessments.
High-Resolution Mass Spectrometry and Impurity Profiling
Development of generic PLGA-based ocular products, including generic dexamethasone intravitreal implants, requires demonstration of both Q1 (qualitative) and Q2 (quantitative) sameness relative to the reference listed drug (RLD). Advanced mass spectrometry workflows are therefore essential for precise polymer characterization and trace-level impurity profiling.
FDA draft guidance documents require manufacturers of generic biodegradable implants to extract PLGA directly from the finished dosage form and perform comparative characterization against the RLD. Required characterization parameters include:
- Polymer composition and lactide molar ratio
- Molecular weight distribution (Mw and Mn)
- Polymer architecture, including linear versus branched structures
ResolveMass Laboratories Inc. supports these analytical requirements using advanced High-Resolution Mass Spectrometry (HRMS) platforms, including Orbitrap and Q-TOF analyzers capable of achieving sub-5 ppm mass accuracy.
This extremely high resolving capability enables analytical scientists to distinguish isobaric species that possess identical nominal masses but differ in elemental composition during extractables and leachables analysis involving packaging systems and single-use applicators.
Combining HRMS with liquid chromatography (LC-MS) facilitates structural elucidation of degradation products, quantification of genotoxic nitrosamine impurities, and determination of residual solvent concentrations, thereby supporting compliance with FDA, EMA, and ICH regulatory requirements.
Navigate Generic ANDA Approvals: For comprehensive compliance guidelines regarding extraction and comparison protocols against reference drugs, access our overview on PLGA polymer sameness for ANDA submissions.
Future Outlook for PLGA-Based Ocular Drug Delivery
The future of PLGA-Based Ocular Drug Delivery is expected to involve increasingly sophisticated multifunctional polymer systems, including drug-eluting contact lenses, bioadhesive nanoparticles, and integrated drug-device combination implants. These emerging technologies aim to eliminate complications associated with repeated ocular injections while simultaneously providing highly precise temporal control over therapeutic release profiles.
As research advances from preclinical investigation toward widespread clinical translation, the incorporation of advanced multifunctional materials remains critically important. Combining PLGA with secondary polymeric systems such as thermosensitive hydrogels, mucoadhesive oligosaccharide coatings, and drug-eluting intraocular lenses is expected to significantly expand the therapeutic potential of both hydrophobic and hydrophilic agents.
Ensuring the structural integrity, safety, and regulatory compliance of these increasingly complex formulations will continue to require highly specialized analytical characterization and validation workflows. Researchers seeking expert consultation, custom polymer synthesis, and validated characterization of long-acting ocular formulations may engage specialized service providers through the ResolveMass Laboratories Inc. contact portal:
https://resolvemass.ca/contact/
FAQs on PLGA-Based Ocular Drug Delivery
The lactide-to-glycolide (L) ratio directly affects the hydrophobicity and degradation behavior of PLGA polymers. Lactide units contain methyl side groups that reduce water penetration into the polymer matrix, while glycolide units are more hydrophilic and absorb water more readily. As water diffusion increases, ester bond hydrolysis accelerates, leading to faster polymer degradation. Therefore, PLGA formulations with higher lactide content generally provide slower and more prolonged drug release compared to formulations with balanced 50:50 monomer compositions.
Acid-capped PLGA contains free terminal carboxylic acid groups, whereas ester-capped PLGA contains alkyl ester end groups that reduce polymer reactivity. The free acid groups in acid-capped PLGA attract water more efficiently and promote autocatalytic hydrolysis within the polymer matrix. This internal acidification accelerates degradation and increases drug release rates. In contrast, ester-capped PLGA absorbs water more slowly, resulting in improved structural stability, reduced burst release, and a more controlled long-term drug delivery profile.
Ozurdex utilizes a biodegradable PLGA matrix that encapsulates 700 µg of dexamethasone within a solid intravitreal implant. After administration into the vitreous cavity, water gradually penetrates the polymer structure and initiates hydrolysis of the ester backbone. Drug release initially occurs through diffusion across the hydrated polymer network and later through gradual bulk erosion of the PLGA matrix. As the implant degrades into lactic acid and glycolic acid monomers, dexamethasone continues to be released over several months in a sustained manner.
PLGA microspheres injected into the vitreous cavity possess a very high surface-area-to-volume ratio, which increases their interaction with immune cells. Macrophages recognize these free particles as foreign materials and initiate phagocytosis, resulting in chronic inflammatory responses. This immune activation stimulates the release of inflammatory cytokines such as TNF-$\alpha$ and IL-6, which contribute to vitritis and vitreous haze. In comparison, solid monolithic PLGA implants with lower exposed surface areas are generally much better tolerated by ocular tissues.
Phase-inversion PLGA implants are injectable liquid formulations composed of PLGA dissolved in water-miscible organic solvents such as N-methyl-2-pyrrolidone (NMP). Once injected into ocular tissue, rapid solvent exchange occurs between the formulation and surrounding physiological fluids. The solvent diffuses outward while water simultaneously enters the polymer solution, causing thermodynamic instability and polymer precipitation. This process transforms the liquid formulation into a solid drug depot that gradually releases the encapsulated therapeutic agent over an extended period.
The initial burst release can be significantly reduced by incorporating drug-loaded PLGA microspheres into a secondary hydrogel matrix. Hydrogels such as poly(acrylamide-sodium acrylate) function as diffusion barriers that slow water penetration into the microspheres. This delayed hydration reduces rapid dissolution of surface-associated drug molecules immediately after administration. As a result, the drug release profile becomes more controlled and prolonged, often extending therapeutic duration several-fold compared with standalone microsphere formulations.
Gamma radiation delivers high-energy ionizing particles that break the ester bonds present within the PLGA polymer backbone. This process, known as chain scission, reduces the polymer’s weight-average molecular weight (Mw) and lowers its glass transition temperature (Tg). Because degradation occurs more rapidly in lower molecular weight polymers, gamma sterilization can alter drug release kinetics and accelerate implant erosion. Excessive radiation exposure may therefore compromise the long-term stability and performance of PLGA-based ocular systems.
Vaporized Hydrogen Peroxide (VHP) sterilization is considered gentler for PLGA-based materials because it primarily sterilizes the surface without deeply penetrating the polymer structure. Unlike Ethylene Oxide (EO), VHP does not significantly plasticize or deform the polymer matrix. EO exposure may cause swelling, shrinkage, or structural distortion of porous PLGA systems due to gas absorption. In contrast, VHP generally preserves polymer morphology, mechanical strength, porosity, and molecular integrity, making it more suitable for sensitive biodegradable ocular implants.
Reference:
- Sharma, S., Parmar, A., Kori, S., & Sandhir, R. (2024). PLGA-The smart biocompatible polymer: Kinetic degradation studies and active principle release. Polymers, 16(3), Article 421. https://doi.org/10.3390/polym16030421
- Makadia, H. K., & Siegel, S. J. (2011). Poly lactic-co-glycolic acid (PLGA) as biodegradable controlled drug delivery carrier. Polymers, 3(3), 1377–1397. https://doi.org/10.3390/polym3031377
- Makadia, H. K., & Siegel, S. J. (2011). Poly lactic-co-glycolic acid (PLGA) as biodegradable controlled drug delivery carrier. Polymers, 3(3), 1377–1397. https://doi.org/10.3390/polym3031377
- Yasukawa, T., Ogura, Y., Sakurai, E., Tabata, Y., & Kimura, H. (2005). Intraocular sustained drug delivery using implantable polymeric devices. Advanced Drug Delivery Reviews, 57(14), 2033–2046. https://doi.org/10.1016/j.addr.2005.09.010
- Yellepeddi, V. K., & Palakurthi, S. (2016). Recent advances in topical ocular drug delivery. Journal of Ocular Pharmacology and Therapeutics, 32(2), 67–82. https://doi.org/10.1089/jop.2015.0047
- Mietzner, R., Kade, C., Froemel, F., Pauly, D., Stamer, W. D., Ohlmann, A., Wegener, J., Fuchshofer, R., & Breunig, M. (2020). Fasudil loaded PLGA microspheres as potential intravitreal depot formulation for glaucoma therapy. Pharmaceutics, 12(8), 706. https://doi.org/10.3390/pharmaceutics12080706

