
Introduction:
PLGA for pulmonary drug delivery has become a focal point for formulators seeking to extend the therapeutic window of inhaled drugs while minimizing systemic side effects. Poly(lactic-co-glycolic acid), or PLGA, for parenteral use is a biodegradable, biocompatible copolymer that has been used for decades in injectable and implantable drug delivery systems. Its extension into the pulmonary space allows drug developers to combine the deep-lung targeting of inhalation therapy with the sustained-release kinetics PLGA is already known for across other long-acting injectable drug delivery technologies. This is particularly valuable for chronic respiratory conditions like asthma, COPD, and pulmonary fibrosis, as well as for systemic drug absorption via the highly vascularized alveolar surface. This article breaks down how PLGA is engineered into inhalable microparticles, the formulation science behind dry powder inhalers, and what the current FDA and EMA regulatory landscape looks like for developers bringing these products to market.
Summary:
- PLGA for pulmonary drug delivery enables sustained-release inhalable microparticles that reduce dosing frequency for respiratory and systemic therapies.
- Particle size (1–5 µm aerodynamic diameter) is the critical quality attribute governing deep lung deposition.
- Dry powder inhaler (DPI) formulations dominate PLGA pulmonary development due to stability advantages over nebulized suspensions.
- Spray drying and spray freeze-drying are the leading manufacturing methods for producing respirable PLGA microparticles.
- FDA and EMA require extensive aerodynamic, degradation, and biocompatibility characterization before IND/CTA filing.
- ResolveMass Laboratories supports PLGA inhalable formulation development with particle characterization, in vitro release testing, and regulatory-ready analytical packages.
1: Why Use PLGA in Inhalable Formulations?
PLGA is used in inhalable formulations because it degrades predictably into lactic and glycolic acid through a process best understood as bulk erosion versus surface erosion in PLGA, allows tunable drug release over days to weeks, and has an established safety record in approved parenteral products. This predictability lets formulators design a single inhaled dose that maintains therapeutic drug levels in lung tissue far longer than a conventional nebulized or immediate-release DPI product. The role of PLGA polymer grade in long-acting release formulation is central to achieving this predictability, since even small shifts in polymer composition can significantly change release behavior.
Key advantages of PLGA microparticles for pulmonary applications include:
- Sustained local or systemic release, reducing dosing frequency from multiple times daily to weekly or less
- Tunable degradation kinetics by adjusting the lactide:glycolide ratio and molecular weight, informed by PLGA glass transition temperature behavior
- Reduced systemic exposure compared to oral or injectable routes, since drug is deposited directly at the site of action
- High drug loading potential, including for formulating highly potent APIs using PLGA microspheres
- Established regulatory precedent, since PLGA is already present in several FDA-approved long-acting injectables, as demonstrated in PLGA characterization of Lupron Depot and related reverse engineering of PLGA polymer in Lupron Depot work
- Compatibility with both small molecules and biologics, including PLGA peptide delivery and broader characterization of long-acting biologics
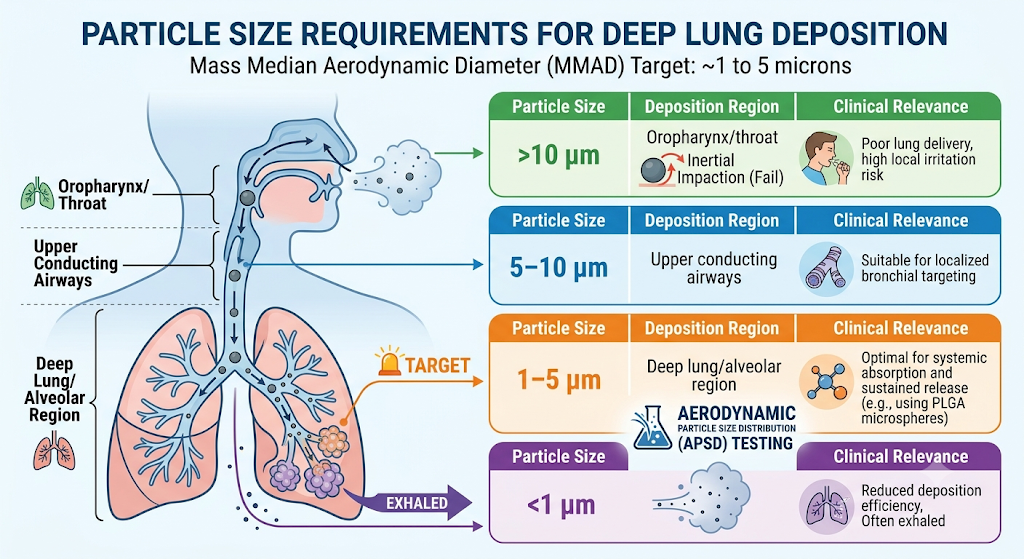
2: What Particle Size Is Required for Deep Lung Deposition?
Effective pulmonary deposition requires a mass median aerodynamic diameter (MMAD) between approximately 1 and 5 microns. Particles larger than 5 microns tend to deposit in the oropharynx and upper airways, while particles smaller than 1 micron are often exhaled before they can settle in the alveolar region.
| Particle Size (MMAD) | Deposition Region | Clinical Relevance |
|---|---|---|
| >10 µm | Oropharynx/throat | Poor lung delivery, high local irritation risk |
| 5–10 µm | Upper conducting airways | Suitable for localized bronchial targeting |
| 1–5 µm | Deep lung/alveolar region | Optimal for systemic absorption and sustained release |
| <1 µm | Often exhaled | Reduced deposition efficiency |
Achieving this narrow particle size window consistently at manufacturing scale is one of the primary formulation challenges in PLGA pulmonary drug development, which is why aerodynamic particle size distribution (APSD) testing via cascade impaction is a non-negotiable analytical step. Understanding the distinction between PLGA nanoparticles vs microspheres is also important at this stage, since particle architecture directly influences both aerodynamic behavior and release kinetics.
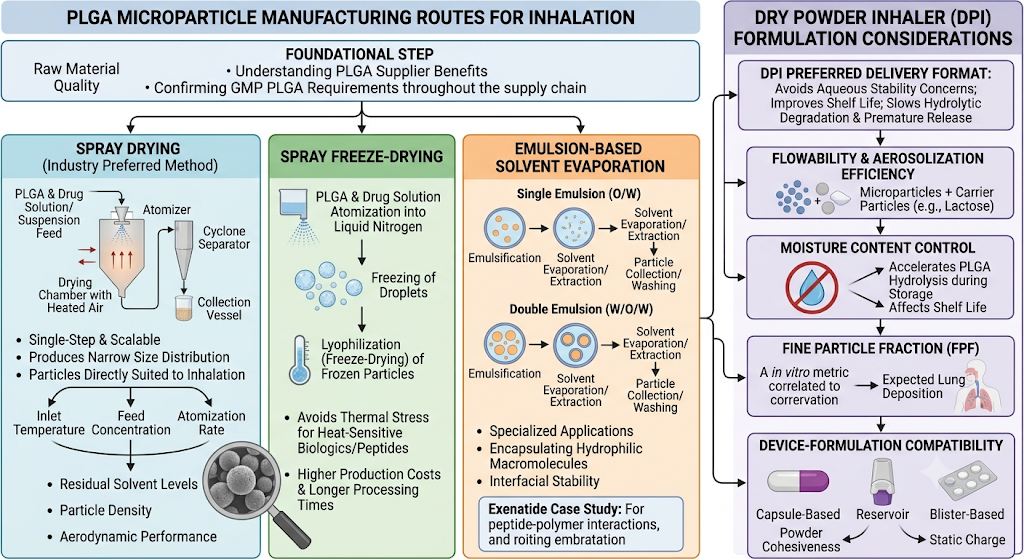
3: How Are PLGA Microparticles Manufactured for Inhalation?
PLGA microparticles for inhalation are most commonly manufactured using spray drying, followed by spray freeze-drying and emulsion-based solvent evaporation for specialized applications. Each method offers a different balance of particle morphology control, drug loading efficiency, and scalability, and general principles of PLGA microsphere formulation development apply across all three approaches.
Spray drying remains the industry-preferred method because it is a single-step, scalable process that produces particles with a narrow size distribution directly suited to inhalation. Process parameters such as inlet temperature, feed concentration, and atomization rate directly influence residual solvent levels, particle density, and aerodynamic performance.
Spray freeze-drying is often selected for heat-sensitive biologics or peptide-loaded PLGA systems, since it avoids the thermal stress associated with conventional spray drying, though it typically involves higher production costs and longer processing times.
Emulsion solvent evaporation (single or double emulsion) is used less frequently for inhalation-ready particles but remains relevant for encapsulating hydrophilic macromolecules where interfacial stability during formation is critical, as illustrated in the exenatide PLGA microsphere characterization case study on overcoming peptide-polymer interaction challenges.
Regardless of manufacturing route, consistent output depends heavily on raw material quality, which is why understanding PLGA supplier benefits and confirming GMP PLGA requirements are upheld throughout the supply chain is a foundational step before formulation work begins.
Dry Powder Inhaler (DPI) Formulation Considerations
DPI formulation is the preferred delivery format for PLGA pulmonary products because it avoids the aqueous stability concerns associated with nebulized suspensions and improves shelf life. Since PLGA is prone to hydrolytic degradation in aqueous environments, formulating as a dry powder significantly slows premature polymer breakdown and drug release prior to administration.
Formulation variables that require careful optimization in PLGA DPI development include:
- Flowability and aerosolization efficiency, often improved through the addition of carrier particles like lactose
- Moisture content control, since residual water accelerates PLGA hydrolysis during storage and directly affects the shelf life of PLGA, PLA, and PCL based products
- Fine particle fraction (FPF), a key in vitro performance metric correlating with expected lung deposition
- Device-formulation compatibility, as capsule-based, reservoir, and blister-based DPI devices each interact differently with powder cohesiveness and static charge
4: What Analytical Testing Supports PLGA Inhalable Development?
PLGA inhalable products require aerodynamic particle size distribution testing, in vitro drug release (IVRT) studies, residual solvent analysis, and polymer characterization including molecular weight and lactide:glycolide ratio confirmation. These analytical packages form the backbone of both formulation optimization and regulatory submission data, and align closely with established PLGA characterization methods used across the broader PLGA product landscape.
Common analytical methods applied to PLGA pulmonary formulations include:
- Cascade impaction (Next Generation Impactor/Andersen Cascade Impactor) for APSD
- Gel permeation chromatography (GPC/SEC) for PLGA molecular weight and polydispersity, part of the broader characterization methods for PLGA microspheres
- HPLC and LC-MS for drug content, related substances, and degradation product quantification
- Residual solvent testing by GC-MS per ICH Q3C guidance
- In vitro release testing under biorelevant or simulated lung fluid conditions
- DSC for glass transition temperature and polymer thermal behavior
5: Regulatory Landscape: FDA and EMA Expectations
Both the FDA and EMA require robust characterization of PLGA-based inhalable products due to the complexity of demonstrating consistent aerodynamic performance and controlled drug release from a biodegradable polymer matrix. Neither agency has a dedicated guidance specific to PLGA inhalation products, so sponsors typically build submissions around existing orally inhaled and nasal drug product (OINDP) guidance combined with long-acting/extended-release product expectations. Generic developers face additional considerations around PLGA reverse engineering for ANDA submissions, including demonstrating PLGA polymer sameness for ANDA filings, work often supported through a specialized PLGA reverse engineering CRO partner offering PLGA polymer characterization for generics.
| Regulatory Consideration | FDA Expectation | EMA Expectation |
|---|---|---|
| Aerodynamic characterization | Cascade impaction data across product shelf life | Cascade impaction plus device-specific performance data |
| Polymer characterization | Molecular weight, LA:GA ratio, end-group chemistry | Comparable polymer CQAs plus batch-to-batch consistency |
| In vitro-in vivo correlation | Encouraged for extended-release claims | Often required for sustained-release justification |
| Impurity/degradation profiling | ICH Q3B/Q3C aligned | ICH-aligned, with added EU pharmacopoeial methods |
| Device compatibility | Combination product pathway may apply | Combination product/medical device interface review |
Because PLGA degrades into lactic and glycolic acid over time, sponsors must also demonstrate that degradation byproducts do not cause local irritation or inflammation in lung tissue, an area regulators scrutinize closely given the sensitivity of pulmonary epithelium compared to other administration routes. Understanding PLGA, PLA, and PCL degradation rate comparisons alongside comprehensive PLGA biocompatibility, safety, toxicology, and regulatory data is essential to building a defensible submission package.
6: PLGA Expertise Across Other Delivery Routes
Pulmonary delivery is one of several administration routes where PLGA’s tunable degradation and biocompatibility profile deliver value. ResolveMass Laboratories’ experience spans a broad range of PLGA-based applications, including:
- PLGA for oncology implants delivering localized, sustained chemotherapeutic release
- Dexamethasone implant PLGA characterization case study work for ocular and localized applications
- PLGA-based ocular drug delivery systems for sustained intraocular therapy
- PLGA in CNS drug delivery and blood-brain barrier applications
- Leuprolide depot formulation challenges and goserelin PLGA implant characterization for hormone-responsive cancer therapies
- Buprenorphine depot PLGA characterization addressing high drug load challenges in long-acting injectables
- Reverse engineering of risperidone PLGA microspheres for generic long-acting antipsychotic development
This cross-platform experience with PLGA across implants, depots, ocular systems, and now inhalable microparticles informs a more robust, risk-aware approach to pulmonary formulation development.
Conclusion:
PLGA for pulmonary drug delivery offers a compelling pathway for extending dosing intervals and improving patient adherence in respiratory and systemic inhaled therapies, but success depends on tightly controlled particle engineering, rigorous analytical characterization, and alignment with FDA and EMA expectations from the earliest stages of development. From spray-dried microparticle production to aerodynamic and polymer characterization, every step requires precision analytical support to move a PLGA pulmonary candidate from bench to clinic with a defensible regulatory package.
Frequently Asked Questions:
PLGA is considered an ideal polymer for inhalable drug delivery because it is biocompatible, biodegradable, and well-established in pharmaceutical applications. After administration, it gradually degrades into lactic acid and glycolic acid, which are naturally eliminated by the body. PLGA protects encapsulated drugs from degradation while enabling controlled and sustained release directly in the lungs. Its physicochemical properties can be tailored by adjusting the polymer composition and molecular weight to achieve desired release profiles. Additionally, PLGA is compatible with several manufacturing techniques, including spray drying, making it suitable for developing inhalable microparticles for respiratory diseases.
The ratio of lactic acid to glycolic acid in PLGA significantly influences the degradation rate and drug release profile. PLGA with a 50:50 ratio generally degrades faster, providing quicker drug release, while polymers with higher lactic acid content, such as 75:25 or 85:15, degrade more slowly and offer prolonged release. Selecting the appropriate polymer ratio allows formulation scientists to match the therapeutic needs of different respiratory diseases. The polymer composition also affects mechanical strength, moisture sensitivity, and stability of inhalable microparticles. Optimizing the PLGA ratio is therefore an important part of formulation development.
Yes. PLGA microparticles can improve patient compliance by providing controlled and sustained drug release, reducing the need for frequent dosing. For patients with chronic respiratory conditions such as asthma or COPD, fewer inhalations may improve treatment adherence. Localized delivery to the lungs also helps achieve therapeutic drug concentrations while potentially reducing systemic side effects. In addition, dry powder inhalers are portable, easy to use, and do not require refrigeration or complex preparation. Together, these advantages contribute to a more convenient treatment experience and better long-term disease management.
PLGA microparticles can encapsulate a broad range of therapeutic molecules, including small-molecule drugs, antibiotics, corticosteroids, peptides, proteins, vaccines, nucleic acids, and anticancer agents. The polymer matrix protects sensitive compounds from environmental degradation while enabling controlled release after inhalation. PLGA is also suitable for both hydrophobic and certain hydrophilic drugs through optimized formulation strategies. This versatility makes it valuable for developing treatments for respiratory diseases as well as systemic therapies delivered through the lungs. Drug selection depends on the desired release profile and formulation requirements.
PLGA microparticles protect sensitive drugs by encapsulating them within a biodegradable polymer matrix that shields them from moisture, oxygen, enzymes, and other environmental factors. This protection helps maintain drug stability during manufacturing, storage, and administration. Encapsulation can also minimize premature drug degradation before reaching the target site in the lungs. As the polymer slowly degrades, the drug is released in a controlled manner, improving therapeutic effectiveness. This protective capability is particularly valuable for biologics, peptides, and other unstable pharmaceutical compounds.
PLGA microparticles and liposomes are both drug delivery systems, but they differ in composition and release behavior. PLGA microparticles are polymer-based carriers that provide long-term controlled drug release through gradual polymer degradation. Liposomes are lipid-based vesicles that encapsulate drugs within phospholipid bilayers and are often used for rapid or targeted drug delivery. PLGA formulations generally offer greater structural stability and prolonged release, while liposomes may provide better compatibility for certain biological molecules. The choice depends on the therapeutic objective, drug properties, and desired release profile.
Aerosol performance is evaluated by measuring how efficiently inhalable particles are delivered to the lungs. Important parameters include Mass Median Aerodynamic Diameter (MMAD), Fine Particle Fraction (FPF), emitted dose, delivered dose uniformity, and aerodynamic particle size distribution. Instruments such as the Andersen Cascade Impactor or Next Generation Impactor (NGI) are commonly used to assess particle deposition characteristics. These tests help determine whether the formulation can reach the deep lung effectively. Consistent aerosol performance is essential for ensuring therapeutic efficacy and meeting regulatory expectations.
Aerodynamic particle size is more important because it determines how particles behave during inhalation and where they deposit within the respiratory tract. Unlike geometric size, aerodynamic diameter considers particle density, shape, and settling characteristics. Particles with an aerodynamic diameter between 1 and 5 µm are generally considered optimal for deep lung deposition. Even particles with similar geometric sizes may behave differently if their densities vary. Therefore, aerodynamic particle size is a key quality attribute for inhalable PLGA formulations and is routinely evaluated during product development.
Yes. PLGA-based inhalation systems deliver drugs directly to the lungs, allowing higher local drug concentrations while reducing systemic exposure. This targeted delivery approach can minimize adverse effects associated with oral or injectable therapies. Controlled drug release from PLGA microparticles further helps maintain therapeutic levels over an extended period without requiring high doses. Lower systemic absorption may improve the overall safety profile for many respiratory treatments. However, the extent of side effect reduction depends on the drug’s properties, formulation design, and clinical application.
Several excipients are used to improve the performance of PLGA dry powder formulations. Common examples include L-leucine, which enhances powder dispersibility; mannitol and trehalose, which improve stability; and lactose, which is widely used as a carrier in dry powder inhalers. Amino acids and other stabilizers may also be incorporated to optimize moisture resistance and aerosolization. The choice of excipients depends on the drug properties, manufacturing process, and intended inhaler device. Proper excipient selection contributes to better stability, flowability, and lung deposition.
Reference
- Encinas-Basurto D, Eedara BB, Mansour HM. Biocompatible biodegradable polymeric nanocarriers in dry powder inhalers (DPIs) for pulmonary inhalation delivery. Journal of Pharmaceutical Investigation. 2024 Mar;54(2):145-60.https://link.springer.com/article/10.1007/s40005-024-00671-0
- Soni SJ. Review on advanced drug delivery systems: innovations in formulation and delivery technologies. The Journal of Multidisciplinary Research. 2024 Nov 2:6-13.https://saapjournals.org/index.php/tjmdr/article/view/635
- Encinas-Basurto D, Martinez-Flores PD, García J, Lopez-Mata MA, García-González G, Rodea GE, Eedara BB, Mansour HM, Juarez J. Latest Advances in Inhalable Dry Powder Bacteriophage Therapy for Pulmonary Infections. Pharmaceutics. 2025 Aug 20;17(8):1077.https://pmc.ncbi.nlm.nih.gov/articles/PMC12389686/
- Zellnitz-Neugebauer S, Fröhlich E. Combinations of Drugs for Pulmonary Inhalation: A Review of Novel Technologies and Toxicological Evaluation Using Cellular Models. Sci. 2026 Apr 14;8(4):89.https://www.mdpi.com/2413-4155/8/4/89
- Chan JG, Wong J, Zhou QT, Leung SS, Chan HK. Advances in device and formulation technologies for pulmonary drug delivery. Aaps Pharmscitech. 2014 Aug;15(4):882-97.https://link.springer.com/article/10.1208/s12249-014-0114-y
- Chakraborty A, Mahar R, Nainwal N. Dry Powder Inhaler of Sustained-Release Microspheres Containing Glycyrrhizin: Factorial Design and Optimization. Combinatorial Chemistry & High Throughput Screening. 2025.https://www.benthamdirect.com/content/journals/cchts/10.2174/0113862073333147250127053403

