
Introduction
The Biosimilar Interchangeability Designation in the USA represents a significant legal and regulatory framework established under the Biologics Price Competition and Innovation Act (BPCIA) of 2009 to enable pharmacy-level substitution of biological therapies. This specific regulatory designation permits pharmacists to substitute an approved interchangeable biosimilar for its reference product without requiring direct intervention from the prescribing healthcare provider, similar to the substitution model used for traditional small-molecule generic drugs. Although standard biosimilars have already demonstrated comparable safety, purity, and potency profiles, obtaining the Biosimilar Interchangeability Designation in the USA provides a distinct market access benefit, especially within retail pharmacy dispensing channels.
Biological products represent a major commercial segment within the modern pharmaceutical industry, accounting for nearly 46% of total therapeutic spending in the United States while representing only approximately 2% of all written prescriptions. Since biological drugs are developed and manufactured using complex living host systems, producing exact copies of these molecules is scientifically unachievable. Therefore, the FDA requires comprehensive analytical, nonclinical, and clinical assessments to confirm that a proposed biosimilar does not have clinically meaningful differences compared with its reference product. This report evaluates the changing regulatory expectations for interchangeability, the evolution of FDA requirements related to clinical switching studies, the complex legal framework governing first-filer market exclusivity, and the direct influence of state-level substitution regulations on commercial market access.
Early Development Tip: Optimizing host platforms during early development stages is critical to preventing downstream structural anomalies. Explore how cell line decisions impact development early on: Learn more about cell line development for biosimilars.
Share via:
Article Summary:
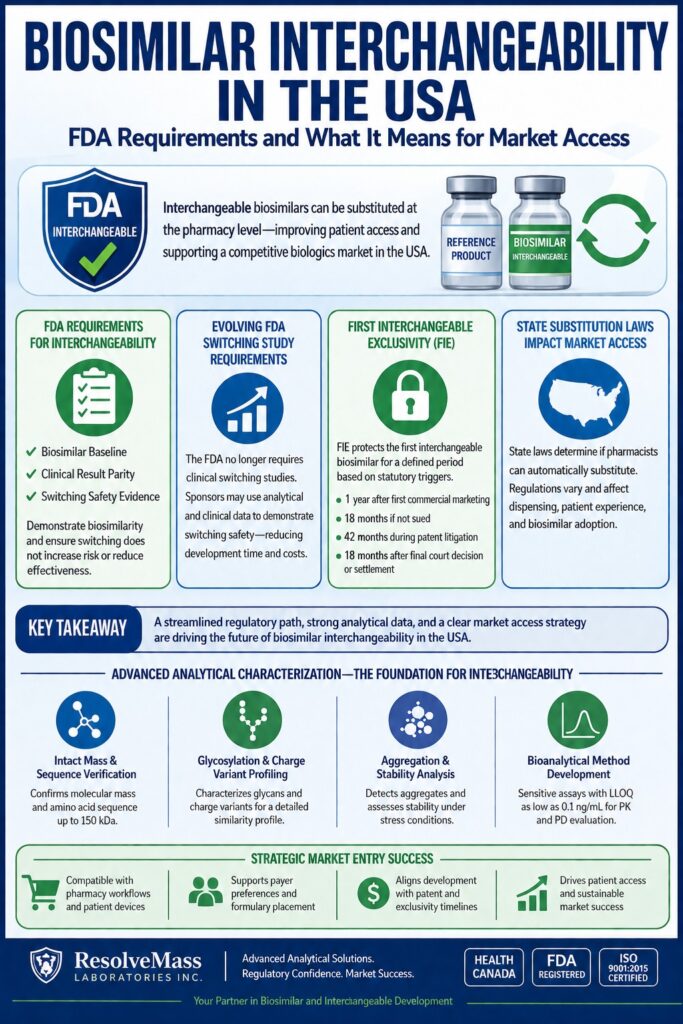
- FDA interchangeability allows pharmacists in the United States to substitute an interchangeable biosimilar for its reference biologic without contacting the prescriber, improving patient access and supporting broader biosimilar adoption.
- Regulatory expectations have evolved, with the FDA now placing greater emphasis on robust analytical and scientific evidence instead of routine clinical switching studies, helping reduce development timelines and overall costs.
- Interchangeability builds on biosimilarity by requiring evidence that patients can switch between the biosimilar and reference product without compromising safety, effectiveness, or immunogenicity.
- First Interchangeable Exclusivity (FIE) offers an important commercial advantage for the first approved interchangeable biosimilar, although the duration depends on market launch timing, patent litigation, and other statutory conditions.
- State-level substitution laws significantly influence real-world market access, as pharmacy substitution rules, prescriber notification requirements, patient consent policies, and record-keeping obligations differ across U.S. states.
- Comprehensive analytical characterization—including molecular structure verification, glycosylation profiling, aggregation analysis, and validated bioanalytical testing—has become the foundation for demonstrating interchangeability and meeting regulatory expectations.
- A successful commercialization strategy requires more than regulatory approval; developers must also consider patent strategy, delivery device compatibility, payer reimbursement, and state substitution regulations to maximize market penetration and long-term success.
FDA Requirements for the Biosimilar Interchangeability Designation in the USA
To achieve the Biosimilar Interchangeability Designation in the USA, a sponsor must establish that the biological product is biosimilar to the reference product and is expected to generate the same clinical outcome in any given patient. According to Section 351(k)(4) of the Public Health Service (PHS) Act, the regulatory standard specifies that for products administered more than once, the potential risk associated with alternating or switching between the proposed interchangeable product and the reference product must not exceed the risk associated with continuous treatment using only the reference product.
The FDA reviews interchangeable biological products through a comprehensive, multi-level evaluation framework. While approval of a standard biosimilar under Section 351(k) requires extensive comparative characterization demonstrating similarity in safety, purity, and potency, the interchangeable pathway historically required submission of a supplemental Biologics License Application (sBLA) supported by clinical evidence demonstrating switching safety. The primary requirements include:
Biosimilarity Baseline:
Obtaining approval as a standard biosimilar is an essential prerequisite, requiring demonstration of high structural and functional similarity with only minor permissible differences in clinically inactive components.
Clinical Result Parity:
The sponsor must demonstrate that the mechanism of action, dosage form, strength, and route of administration are the same as those of the reference biological product.
Switching Safety Evidence:
The sponsor must provide evidence demonstrating that alternating between the biosimilar and the reference biologic does not result in increased immunogenic responses or reduced therapeutic effectiveness during long-term treatment.
Demonstrating Equivalence: Establishing interchangeability begins with proving baseline safety and efficacy through well-designed comparative trials. Review our foundational framework: Read our guide on biosimilar comparability studies.
The Evolutionary Shift in FDA Switching Study Requirements
The FDA has revised its scientific approach and determined that clinical switching studies are generally no longer necessary to support a demonstration of interchangeability for therapeutic proteins. According to updated draft guidance, sponsors may now provide a scientifically justified assessment based on existing analytical and clinical data to demonstrate switching safety, eliminating the previous requirement for multiple switching cycles in clinical trials.
Historically, the FDA’s 2019 “Interchangeability Guidance” suggested that clinical switching studies, in which patients repeatedly alternated between the reference product and the biosimilar, were important for evaluating potential immunogenicity risks, including the formation of neutralizing antibodies (NAbs). However, systematic reviews and extensive post-marketing pharmacovigilance data have indicated that the likelihood of safety concerns or reduced efficacy after single or repeated switches is clinically insignificant. By reducing these clinical development requirements, the FDA aims to accelerate biosimilar development, improve patient access, and decrease drug development expenses by millions of dollars.
Evolution of Key FDA Regulatory Guidance Documents (2024–2026)
| Document and Release Date | Primary Regulatory Change | Strategic Impact on Sponsors |
|---|---|---|
| Considerations in Demonstrating Interchangeability: Update Draft (June 2024) | Removes the routine recommendation for clinical switching studies and emphasizes comparative analytical assessments along with clinical safety evaluations. | Significantly reduces development timelines and decreases dependence on active human clinical trials. |
| Comparative Efficacy Studies Draft Guidance (October 2025) | Simplifies clinical requirements for comparative efficacy studies (CES) by emphasizing the use of highly sensitive analytical technologies. | Reduces standard clinical development timelines by 1 to 3 years and decreases development costs by an average of 24 million. |
| New and Revised Draft Q&As (Revision 4) (March 2026) | Simplifies clinical pharmacokinetic (PK) requirements and eliminates the previous recommendation for three-way PK studies when non-U.S. comparators are used. | Reduces analytical and clinical testing expenses by up to 50%, resulting in estimated savings of 20 million per program. |
This ongoing regulatory alignment demonstrates that the structural requirements needed to establish standard biosimilarity and interchangeability are becoming increasingly similar. As a result, development efforts are shifting away from traditional clinical endpoints toward advanced, high-resolution analytical characterization approaches.
Regulatory Alignment: Meeting shifting FDA guidelines requires a deep understanding of standard characterization expectations. Align your testing program with regulatory frameworks: Explore the ICH Q6B guidelines for biological characterisation.
First Interchangeable Exclusivity: Statutory Clocks and Legal Precedents
First Interchangeable Exclusivity (FIE) prevents the FDA from approving additional interchangeable biosimilars referencing the same reference product for a specific period, creating a valuable commercial opportunity for sponsors that achieve first-to-market status. Established under Section 351(k)(6) of the PHS Act, the duration of this exclusivity period depends on multiple regulatory, legal, and commercial factors, including the progression of patent litigation under the BPCIA’s “patent dance” framework.
The statutory framework specifies that FIE expires based on the earliest occurrence of several predefined events:
First Interchangeable Exclusivity (FIE) Expiration Clock Triggers
| Statutory Trigger Event | Specific Timeline | Legal Context and Impact |
|---|---|---|
| Commercial Marketing | 1 year (12 months) after the first commercial marketing of the first interchangeable product. | Represents the standard intended exclusivity duration when there are no pre-approval legal disputes or clinical delays. |
| Absence of Patent Litigation | 18 months after initial approval of the interchangeable biosimilar if the sponsor was not sued under the BPCIA. | Results in automatic exclusivity expiration when litigation has not been initiated and commercial launch is delayed. |
| Ongoing Patent Litigation | 42 months after approval of the interchangeable biosimilar when patent litigation remains active. | Provides protection to the sponsor during prolonged legal disputes initiated by the reference product manufacturer. |
| Final Court Decision or Settlement | 18 months after a final court decision involving all patents-in-suit or after formal dismissal of the BPCIA litigation. | Prevents unlimited exclusivity extensions when patent disputes are resolved before commercial launch. |
The practical application of these statutory exclusivity timelines was demonstrated through the significant FDA dispute in late 2023 involving Pfizer and Boehringer Ingelheim concerning interchangeable adalimumab biosimilars referencing Humira. The FDA clarified that First Interchangeable Exclusivity is determined separately for different product strengths and formulations, such as 40 mg/0.8 mL and 10 mg/0.2 mL, rather than providing a single exclusivity period for an entire biological molecule.
Importantly, because Boehringer Ingelheim’s interchangeable Cyltezo received approval but experienced a delayed commercial launch due to patent settlement agreements, the 18-month “not sued” trigger resulted in expiration of its exclusivity period in April and September 2023, before its actual market launch in July 2023. This regulatory precedent demonstrates that FIE does not represent an unconditional commercial guarantee. Instead, sponsors must strategically align regulatory approval timelines with patent litigation outcomes and settlement agreements to maximize commercial benefits.
State Substitution Laws and Their Direct Impact on Market Access
State biological substitution laws determine whether pharmacists are permitted to automatically substitute an interchangeable biological product during the dispensing process. While federal interchangeability designation by the FDA confirms therapeutic equivalence between the biosimilar and reference product, the authority to implement substitution at the point of dispensing is entirely governed by individual state legislatures and pharmacy regulatory boards. These state-specific regulations create different levels of administrative complexity that can significantly influence the clinical uptake and commercial adoption of interchangeable biological therapies.
A comprehensive evaluation of biological substitution regulations across all 50 U.S. states, the District of Columbia, and Puerto Rico identifies several key regulatory areas that affect substitution practices and pharmacy workflows:
Key Domains of State-Level Biological Substitution Statutes
| Statutory Domain | Description of Legal Requirement | Impact on Substitution & Market Adoption |
|---|---|---|
| Prescriber Opt-Out (All States) | Prescribers have the authority to prevent automatic substitution by including instructions such as “Dispense as Written” (DAW) or “Brand Medically Necessary” on the prescription. | Maintains physician control over treatment decisions; however, it may also be used by reference product manufacturers to preserve brand loyalty and limit biosimilar adoption. |
| Active Approval Statutes (~10% of States) | Pharmacists are required to obtain direct authorization or approval from the prescribing healthcare provider before dispensing an interchangeable biological product. | Considerably reduces substitution frequency by converting automatic substitution pathways into additional approval-based processes. |
| Physician Notification (~21% of States) | Pharmacists must inform the prescribing physician about the specific biological substitution within a predefined period, generally within 3 to 5 business days. | Creates additional administrative requirements; states with fewer restrictive notification requirements demonstrate a 7.03 percentage point increase in interchangeable product adoption. |
| Patient Notification & Consent (~90% of States) | Pharmacists must notify patients about the substitution at the time of dispensing, with certain states requiring active patient consent before substitution. | May result in patient reluctance when individuals are not adequately informed about biosimilar similarity and therapeutic equivalence. |
| Enhanced Labeling (~44% of States) | Prescription labels must clearly indicate that a biological substitution has occurred. | Improves treatment transparency but may unintentionally create concerns among patients regarding safety or effectiveness. |
| Record Retention (~48% of States) | Pharmacies are required to maintain records of biological substitutions for a legally defined period, generally between 2 and 5 years. | Introduces limited regulatory compliance requirements while supporting standardized tracking of biological substitutions within healthcare systems. |
| Unspecified Legal Liability (~65% of States) | State regulations do not clearly define whether pharmacists assume additional liability when dispensing an interchangeable biological product compared with the reference product. | May create uncertainty among pharmacists and contribute to hesitation due to concerns regarding potential malpractice exposure. |
The commercial importance of these state-level regulatory differences is demonstrated by a cohort study evaluating interchangeable insulin glargine products referencing Lantus. Commercially insured patients located in states with less restrictive substitution policies were 7.03 percentage points more likely to receive interchangeable insulin glargine after its market introduction. Additionally, interchangeability can indirectly accelerate biosimilar adoption through the “coverage channel,” encouraging health insurance plans and pharmacy benefit managers (PBMs) to prioritize interchangeable biological products within preferred formulary positions.
Targeted Development: Navigating state-level substitution variations successfully depends heavily on choosing the right target molecule. Learn more about optimizing high-demand therapeutics: Discover how to navigate insulin biosimilar characterization.
Analytical Characterization and Bioanalytical Method Validation for Interchangeable Products
Demonstrating the structural and functional similarity required for an interchangeable designation depends on the implementation of highly sensitive analytical characterization strategies. Biological therapeutics, including monoclonal antibodies, fusion proteins, and synthetic polypeptides, are produced using complex cellular bioreactor systems and are therefore susceptible to micro-heterogeneity, structural modifications, degradation pathways, and immunogenicity-related variations. To reduce regulatory uncertainty and minimize dependence on extensive clinical efficacy studies, developers must establish comparable critical quality attributes (CQAs) through comprehensive orthogonal analytical testing approaches.
Risk Mitigation: To successfully avoid costly clinical switching studies, developers must map out all relevant molecular variations. Understand molecular variations and how to control them: Understand critical quality attributes (CQAs) in biosimilars.
As a Health Canada-licensed, FDA-registered, and ISO 9001:2015 certified contract research organization, ResolveMass Laboratories Inc. provides advanced analytical testing and validated bioanalytical solutions to support biopharmaceutical developers in biosimilar and interchangeable product development. With a focus on scientific accuracy and regulatory compliance, ResolveMass Laboratories Inc. integrates structural characterization strategies and analytical method validation approaches according to FDA, EMA, and Health Canada regulatory expectations.
Expert Testing Support: Partnering with a specialized lab streamlines your regulatory pathway. Access expert support to streamline your regulatory submissions: Browse our comprehensive biosimilar characterization services today.
State-of-the-Art Analytical Support for Biologics and Biosimilars
Intact Mass & Primary Sequence Verification:
High-resolution accurate mass (HRAM) liquid chromatography-mass spectrometry (LC-MS/MS) techniques are utilized to confirm intact molecular masses up to 150 kDa, ensuring accurate amino acid sequence confirmation while identifying potential structural truncations or modifications.
Structural Modifications: Even minor changes in the primary sequence can lead to substantial alterations in function. Learn how mass spectrometry reveals the complex modifications that impact clinical efficacy: Read about post-translational modifications (PTMs) in biosimilars.
Glycosylation and Charge Variant Profiling:
Advanced analytical approaches are applied to characterize N-linked and O-linked glycans along with acidic and basic charge variants. These attributes are essential for demonstrating a fingerprint-like analytical similarity profile between the proposed interchangeable product and the reference biologic.
Heterogeneity Control: Profiling micro-heterogeneity helps establish biochemical equivalence to the reference product. Fine-tune your profiling with targeted separation techniques: Explore charge variant analysis in biosimilars using mass spectrometry and discover how to optimize your glycosylation analysis of biosimilars.
Aggregation and Stability Analysis:
Size-exclusion chromatography (SEC) and triple-detection gel permeation chromatography (GPC) are employed to identify molecular weight distribution changes, assess formulation stability during forced degradation studies, and reduce the risk of aggregation-associated immunogenic responses.
Formulation Stability: Uncovering physical instability early prevents immunogenicity issues down the line.Evaluate degradation pathways and establish stability profiles under stressed conditions: Learn about forced degradation of biosimilars and delve into aggregation analysis in biosimilars.
Bioanalytical Method Development & Validation:
Customized bioanalytical assays are developed and validated with lower limits of quantification (LLOQ) reaching as low as 0.1 ng/mL. These sensitive methods enable accurate evaluation of pharmacokinetic (PK) and pharmacodynamic (PD) parameters, including AUC and Cmax, across different biological matrices.
Regulatory Compliance & Audit Readiness:
Comprehensive regulatory support is provided through fully validated, GLP-compliant analytical datasets, secure laboratory information management systems (LIMS), and detailed documentation packages designed to support supplemental Biologics License Application (sBLA) and abbreviated Biologics License Application (aBLA) submissions.
Implementing advanced bioanalytical characterization strategies early during the development process helps minimize regulatory challenges and compliance risks. These approaches enable developers to effectively address the complex scientific and regulatory expectations associated with achieving approval through the interchangeable biosimilar pathway.
Strategic Market Entry Under the Biosimilar Interchangeability Designation in the USA
Achieving successful market entry under the Biosimilar Interchangeability Designation in the USA requires a comprehensive commercial strategy that addresses both patient delivery systems and payer formulary placement. Developers must carefully align their clinical development schedules with patent litigation outcomes and settlement agreements while ensuring that the final drug product maintains compatibility with the physical presentation and administration characteristics of the reference biologic.
One of the most important considerations in current market access strategies is “device presentation.” The FDA evaluates container closure systems, including prefilled syringes, prefilled pens, and autoinjectors, as part of the overall interchangeability assessment. For instance, the FDA approved Sandoz’s Hyrimoz prefilled syringes as interchangeable with Humira; however, the autoinjector presentation containing the same strength did not receive interchangeable designation. Since pharmacy-level substitution relies significantly on the ability of patients to transition between products without requiring additional device training, differences in delivery systems may interfere with substitution practices and negatively affect commercial adoption.
Additionally, developers must differentiate between biologic products that are dispensed through retail pharmacies and those administered within clinical settings. For physician-administered therapies covered under a patient’s medical benefit, such as oncology infusion products, pharmacist-driven point-of-sale substitution is generally not applicable from either a legal or practical perspective. Within these therapeutic areas, the interchangeable designation has limited influence on purchasing decisions and clinical implementation. Instead, market success is primarily determined by payer reimbursement strategies, competitive net pricing, and healthcare provider education, making formulary placement a key factor influencing market penetration and product uptake.
Conclusion: The Future of the Biosimilar Interchangeability Designation in the USA
In conclusion, the Biosimilar Interchangeability Designation in the USA is experiencing substantial evolution due to advancements in clinical understanding and the development of a more streamlined regulatory framework. Through the gradual reduction of clinical switching study requirements and simplification of comparative pharmacokinetic evaluations, the FDA is decreasing development costs while accelerating regulatory review timelines. This changing regulatory environment enables biopharmaceutical manufacturers to redirect resources toward advanced analytical characterization strategies, bringing the biologics approval pathway closer to the established model used for small-molecule generic products.
For manufacturers seeking a competitive position within the multi-billion-dollar U.S. biologics market, the regulatory emphasis has transitioned from extensive clinical efficacy investigations toward generating highly precise and comprehensive analytical comparability data. Collaborating with an experienced contract research organization such as ResolveMass Laboratories Inc. provides developers with access to advanced mass spectrometry platforms, customized chromatography solutions, and fully validated bioanalytical workflows. This strong analytical foundation supports compliance with regulatory expectations, facilitates navigation of state-level substitution requirements, and contributes to sustainable commercial success.
To explore how specialized analytical validation strategies and comparative testing workflows can strengthen your biosimilar development program, connect with the scientific experts at ResolveMass Laboratories Inc. through the ResolveMass Laboratories Contact Page.
Frequently Asked Questions (FAQs)
Yes, manufacturers may achieve the Biosimilar Interchangeability Designation in the USA without conducting traditional clinical switching studies under the FDA’s updated regulatory approach. The June 2024 draft guidance indicates that switching studies are generally no longer required when sufficient analytical and clinical evidence is available. Sponsors can provide a scientifically justified assessment demonstrating that switching between the biosimilar and reference product does not introduce additional safety risks or affect therapeutic performance.
First Interchangeable Exclusivity (FIE) is assessed separately for individual product strengths, concentrations, and presentations rather than being granted universally for an entire biological molecule. As a result, different formulations or strengths of the same reference product may receive independent exclusivity periods. For example, a manufacturer may obtain FIE protection for a 40 mg presentation, while another sponsor could potentially qualify for exclusivity for a different 10 mg presentation.
State-specific biological substitution regulations play a major role in determining how quickly interchangeable insulin products are adopted in clinical practice. Restrictive requirements, including additional prescriber approvals and patient consent procedures, can reduce substitution efficiency at pharmacies. Studies evaluating interchangeable insulin glargine demonstrated that patients in states with less restrictive substitution policies were 7.03 percentage points more likely to receive the interchangeable product after market introduction.
The FDA increasingly relies on advanced analytical technologies because they can detect minor structural and functional differences between biological products with greater sensitivity than traditional clinical trials. Techniques such as high-resolution mass spectrometry provide detailed characterization of critical quality attributes that may not be identified through comparative efficacy studies. Analytical approaches also reduce development timelines by avoiding lengthy clinical trials that may require 1 to 3 years and approximately 24 million in additional costs.
The delivery device associated with a biological product is an important factor in the interchangeability evaluation because patients must be able to transition between products safely and effectively. The FDA assesses container closure systems, including prefilled syringes, pens, and autoinjectors, to determine whether device differences could create administration challenges. In some cases, a prefilled syringe may receive interchangeable status while an autoinjector containing the same strength may not qualify due to differences in usability or training requirements.
State biological substitution laws include multiple regulatory requirements that influence pharmacy-level substitution practices. These requirements commonly involve prescriber approval provisions, patient notification or consent obligations, physician communication timelines, prescription labeling requirements, and record retention responsibilities. Variations among states create different levels of administrative burden that can either facilitate or restrict adoption of interchangeable biological products.
Hybrid LC-MS/MS and ligand-binding assays (LBA) provide essential analytical support for demonstrating pharmacokinetic (PK) and pharmacodynamic (PD) similarity between biosimilar and reference biological products. These hybrid methods combine the selectivity of antibody-based extraction with the sensitivity and precision of mass spectrometry-based detection. They enable accurate quantification of therapeutic molecules in complex biological matrices, achieving detection capabilities as low as 0.1 ng/mL.
The FDA has identified potential legislative changes that could modify the current interchangeability framework by removing the separate statutory requirements for interchangeable designation. If such amendments to the Public Health Service (PHS) Act are approved by Congress, all FDA-approved biosimilars could potentially receive automatic interchangeability status. This change would eliminate the current two-tier regulatory system and simplify biosimilar adoption across the healthcare system.
Reference:
- U.S. Food and Drug Administration. (2024). Biosimilar and interchangeable biologics: More treatment choices. U.S. Department of Health and Human Services. https://www.fda.gov/consumers/consumer-updates/biosimilar-and-interchangeable-biologics-more-treatment-choices
- U.S. Food and Drug Administration. (2024). Considerations for demonstrating interchangeability with a reference product: Update (Draft guidance for industry). U.S. Department of Health and Human Services. https://www.fda.gov/media/189366/download
- Kurki, P., Barry, S., Bourges, I., Tsantili, P., & Wolff-Holz, E. (2021). Safety, immunogenicity and interchangeability of biosimilar monoclonal antibodies and fusion proteins: A regulatory perspective. Drugs, 81, 1887–1901. https://doi.org/10.1007/s40265-021-01601-8
- Herndon, T. M., Ausin, C., Brahme, N. N., Schrieber, S. J., Luo, M., Andrada, F. C., Kim, C., Sun, W., Zhou, L., Grosser, S., Yim, S., & Ricci, M. S. (2023). Safety outcomes when switching between biosimilars and reference biologics: A systematic review and meta-analysis. PLOS ONE, 18(10), e0292231. https://doi.org/10.1371/journal.pone.0292231
- U.S. Food and Drug Administration. (2024). FDA moves to accelerate biosimilar development and lower drug costs. U.S. Department of Health and Human Services. https://www.fda.gov/news-events/press-announcements/fda-moves-accelerate-biosimilar-development-and-lower-drug-costs
- U.S. Food and Drug Administration. (2025). New and revised draft Q&As on biosimilar development and the BPCI Act (Revision 4). U.S. Department of Health and Human Services. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/new-and-revised-draft-qas-biosimilar-development-and-bpci-act-revision-4
- U.S. Food and Drug Administration. (2024). 9 things to know about biosimilars and interchangeable biosimilars. U.S. Department of Health and Human Services. https://www.fda.gov/drugs/things-know-about/9-things-know-about-biosimilars-and-interchangeable-biosimilars

