Advanced Extractables & Leachables Testing for Ophthalmic Drug Products
Evaluating extractables and leachables in ophthalmic formulations demands a detailed understanding of polymer semipermeability, formulation behavior, and applicable regulatory expectations. Implementing a structured approach for Extractables & Leachables Testing for Ophthalmic Drug Products is essential for detecting and controlling chemical impurities that may lead to ocular toxicity or affect formulation stability.
Learn about our comprehensive Extractables & Leachables Testing for Ophthalmic Drug Products services here.
Historically, topical ophthalmic solutions and suspensions were categorized alongside parenteral (injectable) drug products under high-risk classification systems because both involve sterile liquid administration. In 2008, the Product Quality Research Institute (PQRI) established the Parenteral and Ophthalmic Drug Product (PODP) Working Group to extend science-based and risk-based safety thresholds initially developed for orally inhaled and nasal drug products (OINDP).
While the group defined a systemic Safety Concern Threshold (SCT) of 1.5 µg/day for injectables, it determined that a single systemic threshold could not be scientifically applied to ophthalmic delivery. The eye is a low-volume, immunologically sensitive organ, where even trace levels of packaging-related impurities can lead to localized irritation, corneal cellular injury, or inflammatory responses. As a result, safety evaluation for ophthalmic products requires localized toxicity assessment rather than systemic daily intake models.
This distinction led to the development of dedicated regulatory frameworks and container-specific chemical characterization approaches. Over time, a baseline reporting expectation of 1 µg/mL (1 ppm) for unknown migrants in ophthalmic stability studies became common practice. These expectations are now reflected in modern regulatory guidance, including the United States Food and Drug Administration (FDA) late 2023 Draft Guidance, which defines concentration-based limits specifically intended to address localized ocular toxicity.
To comply with these expectations, developers must understand how formulation excipients interact with semipermeable polymer systems, how secondary packaging can contribute migrants that penetrate primary containers, and how high-resolution mass spectrometry workflows can be optimized for trace-level impurity detection.
Understand how we establish the AET for Extractables and Leachables Studies.
Share via:
Article Summary:
- Ophthalmic extractables and leachables (E&L) testing focuses on identifying chemical impurities from packaging materials that may cause ocular irritation, toxicity, or stability issues in drug formulations.
- Unlike injectable or inhalation products, ophthalmic drugs require localized safety evaluation because the eye is highly sensitive and cannot rely on traditional systemic exposure-based thresholds.
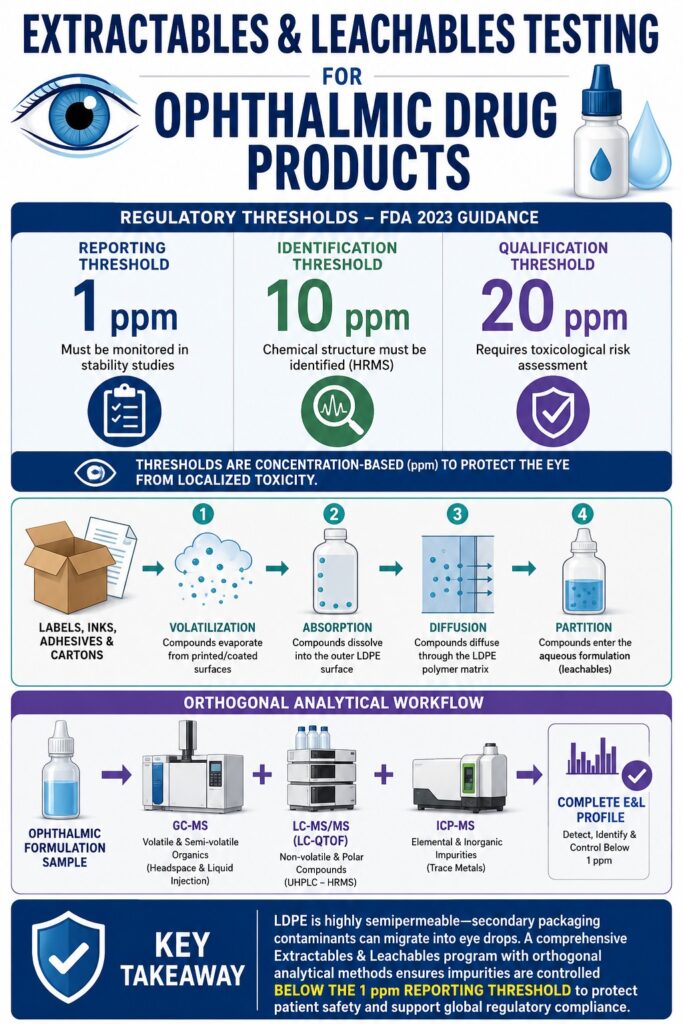
- Regulatory frameworks such as the FDA 2023 guidance use fixed concentration limits—1 ppm (reporting), 10 ppm (identification), and 20 ppm (qualification)—replacing older percentage- or daily-dose-based impurity models.
- Packaging systems, especially semipermeable LDPE containers, can allow migration of additives and contaminants from secondary packaging (inks, adhesives, cartons) into the drug product over time.
- Various analytical tools, including GC-MS, LC-MS/MS, and ICP-MS, are required together to detect volatile, non-volatile, and elemental impurities for a complete E&L profile.
- Polymer additives and formulation interactions (e.g., adsorption of preservatives like BKC or drug loss via hydrophobic interactions) can significantly influence drug stability and safety.
- A structured E&L strategy—covering material science, migration pathways, stability testing, and regulatory thresholds—is essential to ensure compliance and protect patient safety in ophthalmic drug products.
Regulatory Threshold Paradigms for Extractables & Leachables Testing for Ophthalmic Drug Products
Topical ophthalmic drug products are regulated using concentration-based thresholds defined by the FDA, rather than the daily intake Safety Concern Threshold approach used for other dosage forms. The 2023 FDA guidance titled Quality Considerations for Topical Ophthalmic Drug Products defines reporting, identification, and qualification thresholds of 1 ppm, 10 ppm, and 20 ppm, respectively.
These limits represent a major shift from conventional systemic impurity frameworks. Under the International Council for Harmonisation (ICH) Q3B(R2) guideline, impurity limits are expressed as a percentage of the active pharmaceutical ingredient (API). In contrast, the FDA applies fixed limits for ophthalmic products due to the risk of localized ocular toxicity and the limited availability of comprehensive ocular irritation datasets at trace levels.
For drug products with strengths less than or equal to 0.1% w/v, the FDA recommends an identification and qualification threshold of 1% of API strength or 1 ppm, whichever is higher.
The table below compares regulatory threshold frameworks across different high-risk dosage forms, highlighting the unique requirements for ophthalmic products:
Regulatory Threshold Comparison Across Dosage Forms
| Parameter / Threshold Type | Orally Inhaled & Nasal (OINDP) | Parenteral Drug Products (PDP) | Topical Ophthalmic Drug Products (ODP) |
|---|---|---|---|
| Primary Safety Metric | Daily Intake (µg/day) | Daily Intake (µg/day) | Localized Concentration (ppm or µg/g) |
| Reporting Threshold | Derived from SCT ≤ 0.15 µg/day (cite: 25, 26) | Derived from SCT ≤ 1.5 µg/day (cite: 13, 18) | 1 ppm (mass/mass of formulation) |
| Identification Threshold | Derived from SCT ≤ 0.15 µg/day (cite: 18, 26) | Derived from SCT ≤ 1.5 µg/day (cite: 13, 18) | 10 ppm (mass/mass of formulation) |
| Qualification Threshold | 5 µg/day (QT) | 5 µg/day (Adapted Cramer Class) | 20 ppm (mass/mass of formulation) |
| Primary Safety Concerns | Pulmonary toxicity, systemic exposure | Systemic toxicity, blood-contact safety | Localized irritation, corneal damage |
| Regulatory References | PQRI (2006), USP <1664.1> | PQRI (2021), USP | FDA Draft Guidance (2023), USP |
View our guidance on Toxicological Qualification of Leachables.
For a New Drug Application (NDA), Abbreviated New Drug Application (ANDA), or Biologics License Application (BLA), any leachable detected at or above the 1 ppm reporting threshold must be monitored throughout stability studies and documented in the Chemistry, Manufacturing, and Controls (CMC) section.
Learn about Leachables Monitoring during Stability Studies.
If a leachable exceeds the 10 ppm identification threshold, its chemical structure must be fully characterized using high-resolution mass spectrometry. Any compound reaching or exceeding the 20 ppm qualification threshold requires a full toxicological risk assessment, addressing both localized ocular effects and systemic safety endpoints.
Container Closure System Materials and Semipermeability Mechanics
Low-density polyethylene (LDPE) is widely used for ophthalmic squeeze bottles due to its flexibility and processability. However, its low-crystallinity polymer structure makes it highly semipermeable to external organic compounds. This allows volatile and semi-volatile substances from secondary packaging to diffuse through the container walls and enter the sterile formulation.
Explore options for Low-Leachables Packaging Materials.
LDPE consists of a highly branched molecular structure that prevents tight packing of polymer chains into crystalline regions. This creates significant free volume within the material. While this property enables squeezable functionality for multi-dose dropper bottles, it also creates diffusion pathways for small molecules. Organic compounds with molecular weights below 500 Da can readily partition into the polymer, diffuse through the matrix via concentration gradients, and migrate into the aqueous drug product.
Polymer Science and Chemical Compositions in Extractables & Leachables Testing for Ophthalmic Drug Products
Understanding polymer composition is essential for predicting extractable and leachable profiles of both primary and secondary packaging components. Each material contains specific additive systems, such as antioxidants, stabilizers, and slip agents, which may migrate under environmental or formulation stress.
Find details on Solvents for Extractables Studies.
Medical-grade LDPE resins used in blow-fill-seal (BFS) or preformed systems typically require fewer additives compared to more rigid polymers like polyvinyl chloride (PVC) or polycarbonate. However, additives are still incorporated to support processing stability, melt behavior, and long-term durability.
The table below summarizes typical material compositions and associated additives used in ophthalmic container closure systems:
Packaging Materials and Additive Profiles
| Component Material Type | Polymer Matrix / Base | Additives / Vulcanizers | Target Concentrations | Known Extractables / Degradation Products |
|---|---|---|---|---|
| LDPE Blown Film (Primary Resins) (cite: 7, 13) | Low-Density Polyethylene (100%) | Irganox B 215 (antioxidant blend), BHT (antioxidant), calcium stearate (acid scavenger), erucamide (slip agent), Chimassorb 944 (UV stabilizer) | 1000 ppm, 200 ppm, 500 ppm, 500 ppm, 2000 ppm (cite: 13) | Oxidized Irgafos 168, palmitic acid, aliphatic acids, Chimassorb degradation products |
| Bromobutyl Sheet (Closures / Liners) (cite: 13, 33) | Brominated isobutylene isoprene copolymer (57.3%) | Calcined aluminum silicate, titanium dioxide, paraffinic oil, zinc oxide, polyethylene, SRF carbon block mixture | 38.2%, 1.2%, 1.2%, 0.6%, 0.6%, 0.4% (cite: 13) | Elemental zinc, paraffinic oligomers, titanium residues, stearic derivatives |
During manufacturing or high-temperature sterilization, these additives may undergo chemical transformation. For instance, the organophosphite antioxidant Irgafos 168 can oxidize into its phosphate form, which is more polar and migrates more readily into aqueous formulations. Similarly, Chimassorb 944 may degrade under thermal stress, producing low-molecular-weight amine fragments that enter the headspace.
Unstabilized LDPE can also undergo thermo-oxidative chain scission, producing aliphatic carboxylic acids such as palmitic acid, which may influence formulation pH.
Secondary Packaging Migration Mechanics and Empirical Case Studies
Secondary packaging components, including label adhesives, inks, varnishes, and cartons, are often the primary contributors to leachables in ophthalmic drug products. Because LDPE is not an effective barrier to volatile organic compounds, substances from secondary packaging can permeate the primary container over time.
Migration occurs through a multi-step process. First, volatile compounds evaporate from printed or coated surfaces into the surrounding air. Second, they dissolve into the external surface of the LDPE bottle. Third, they diffuse through the polymer matrix. Finally, they partition into the aqueous formulation, where surfactants may enhance solubility and retention.
Learn about the Root Causes of Failed Extractables and Leachables (E&L) Studies.
Empirical Case Studies of Migration in Semipermeable Systems
Case Study 1: Acrylate Ester Migration from Viscosity Modifiers
Acrylate esters are commonly used in UV-cured inks to adjust viscosity. During stability studies of an ophthalmic product in an LDPE bottle, methyl and ethyl acrylate monomers were observed entering the formulation.
These volatile compounds rapidly diffused through the container wall, reaching approximately 0.4 ppm within the first few months. Over six months, levels decreased below 0.2 ppm.
This decline occurred due to volatilization from the primary container into the surrounding environment, establishing a dynamic equilibrium rather than continuous accumulation.
Case Study 2: Polyethylene Glycol (PEG) Related Species from Pressure-Sensitive Adhesives
PEG-related oligomers (400–600 Da) used in pressure-sensitive adhesives were detected during long-term stability studies at 25°C and 40% relative humidity.
Although initially considered non-migratory due to their size and low volatility, these oligomers slowly partitioned into LDPE when labels were in direct contact with the container surface.
Unlike volatile compounds, these PEG species showed a steady, irreversible increase over time. After 18 months, concentrations exceeded the 1.0 ppm threshold. This demonstrated that non-volatile additives can act as persistent long-term leachables.
Analytical Evaluation Threshold Mathematical Formulations and Derivations
The Analytical Evaluation Threshold (AET) defines the concentration at which an extractable or leachable must be identified and evaluated for toxicological risk. Although ophthalmic products follow a regulatory limit of 1 ppm, deriving a system-specific AET remains essential for analytical justification.
To translate systemic safety thresholds into container-specific limits, PQRI methodology is used. This converts a mass-per-day threshold into a concentration-based analytical limit.
For multi-dose systems, the estimated AET in micrograms per gram (µg/g) is calculated as:
AET estimated = (SCT / Doses per Day) × (Total Labeled Doses per CCS / Mass of CCS Component)
When expressed in concentration terms (µg/mL or ppm), the equation becomes:
AET estimated = SCT / MDD
Where:
- SCT is the Safety Concern Threshold, typically 1.5 µg/day for ophthalmic and parenteral systems under PQRI guidelines
- MDD is the Maximum Daily Dose in mL/day
Example:
For a moxifloxacin ophthalmic solution in a 5 mL container with a maximum daily dose of 0.5 mL/day:
AET estimated = 1.5 µg/day ÷ 0.5 mL/day = 3.0 µg/mL = 3.0 ppm
To obtain the final analytical reporting threshold, variability in detector response is considered using an uncertainty factor:
AET final = AET estimated × (1 − UF)
or
AET final = AET estimated ÷ Uncertainty Factor
The uncertainty factor is derived from variability in response factors across reference standards. When variability is high, values between 2 and 10 are applied. Under FDA 2023 guidance, any calculated value above 1 ppm must be reduced to a final reporting threshold of 1.0 ppm.
Formulation Interactions: Preservative Adsorption and Surfactant Extraction Sinks
Ophthalmic formulations often contain complex excipient systems that influence migration behavior. These components can either enhance or inhibit leaching by acting as solubilizers or adsorption sites.
Benzalkonium chloride (BKC) is a common preservative composed of alkylbenzyldimethylammonium chlorides with varying chain lengths. Its amphiphilic nature gives it strong surface activity and affinity for hydrophobic surfaces such as LDPE.
Over time, BKC can adsorb onto container walls, reducing its concentration in the formulation. If this reduction exceeds acceptable limits, antimicrobial effectiveness may be compromised, potentially failing USP requirements and increasing contamination risk.
Adsorption rates under accelerated conditions (60°C and 75% relative humidity for 5 days) vary across materials:
Preservative Adsorption Profiles
LDPE
- Thimerosal: Initial 1.98 mg/mL, recovery 99.76%, adsorption 0.24% (cite: 42)
- Chlorobutanol: Initial 8.80 mg/mL, recovery 88.18%, adsorption 11.82% (cite: 42)
- Benzalkonium Chloride (BKC): Initial 10.56 mg/mL, recovery 98.53%, adsorption 1.47% (cite: 42)
- Propylparaben: Initial 3.98 mg/mL, recovery 96.64%, adsorption 3.36% (cite: 42)
- Phenoxyethanol: Initial 2.49 mg/mL, recovery 95.48%, adsorption 4.52% (cite: 42)
Polypropylene (PP)
- Thimerosal: Initial 1.98 mg/mL, recovery 100%, adsorption 0% (cite: 42)
- Chlorobutanol: Initial 8.80 mg/mL, recovery 87.47%, adsorption 12.53% (cite: 42)
- Benzalkonium Chloride (BKC): Initial 10.56 mg/mL, recovery 99.31%, adsorption 0.69% (cite: 42)
- Propylparaben: Initial 3.98 mg/mL, recovery 98.18%, adsorption 1.82% (cite: 42)
- Phenoxyethanol: Initial 2.49 mg/mL, recovery 94.61%, adsorption 5.39% (cite: 42)
Polyethylene Terephthalate (PET)
- Thimerosal: Initial 1.98 mg/mL, recovery 99.92%, adsorption 0.08% (cite: 42)
- Chlorobutanol: Initial 8.80 mg/mL, recovery 98.61%, adsorption 1.39% (cite: 42)
- Benzalkonium Chloride (BKC): Initial 10.56 mg/mL, recovery 99.84%, adsorption 0.16% (cite: 42)
- Propylparaben: Initial 3.98 mg/mL, recovery 96.25%, adsorption 3.75% (cite: 42)
- Phenoxyethanol: Initial 2.49 mg/mL, recovery 94.28%, adsorption 5.72% (cite: 42)
While thimerosal shows minimal interaction across materials, chlorobutanol exhibits higher adsorption, particularly in LDPE and PP systems. This highlights the importance of careful preservative compatibility studies during packaging selection.
In addition, active pharmaceutical ingredients may also interact with container surfaces. Prostaglandin analogs used in glaucoma treatment, such as latanoprost, are highly hydrophobic and may adsorb onto LDPE surfaces, leading to potency loss.
To reduce this effect, surfactants are often included to form micelles around hydrophobic drug molecules. However, these micelles may also enhance leaching by solubilizing hydrophobic additives from the polymer matrix, effectively acting as extraction sinks. Therefore, formulation-specific micellar behavior must be considered during E&L assessment.
Advanced Analytical Methodologies and Orthogonal Screening Workflows
Detecting trace-level impurities in ophthalmic systems requires a combination of gas chromatography, liquid chromatography, and plasma mass spectrometry techniques. No single method is sufficient to capture the full range of potential extractables and leachables.
A multi-platform workflow is therefore required:
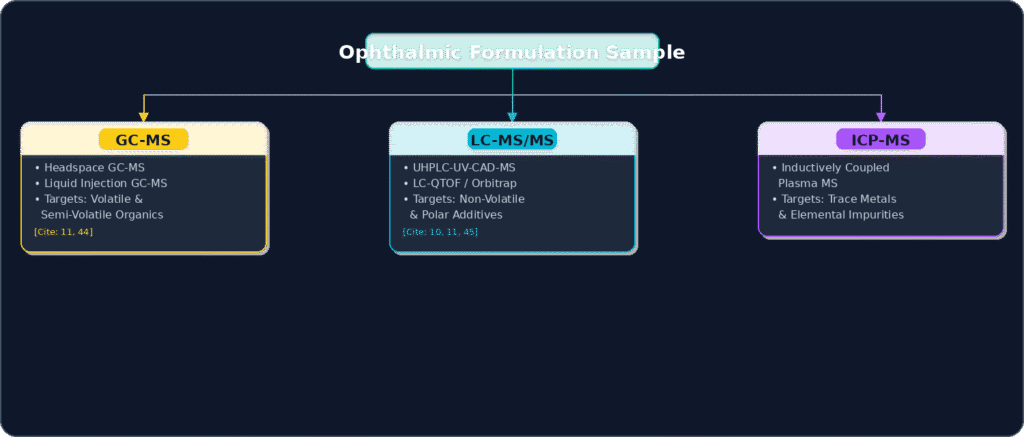
Gas Chromatography-Mass Spectrometry (GC-MS)
GC-MS is used for volatile and semi-volatile organic compounds. Headspace GC-MS is applied for residual solvents and volatile ink components, while liquid injection GC-MS/MS targets compounds such as slip agents and antioxidants. Spectral deconvolution tools such as AMDIS help resolve overlapping peaks and match spectra with reference libraries.
Liquid Chromatography-Tandem Mass Spectrometry (LC-MS/MS and LC-QTOF)
LC-MS/MS and high-resolution LC systems are used for non-volatile compounds, including phenolic antioxidants and polymer additives. UHPLC combined with QTOF or Orbitrap instruments enables untargeted screening and structural identification. Dual ionization modes (positive and negative electrospray ionization) ensure detection across acidic, basic, and neutral species.
Inductively Coupled Plasma Mass Spectrometry (ICP-MS)
ICP-MS is the preferred technique for detecting trace metals and inorganic impurities. It is used to identify elemental leachables such as zinc, calcium, and aluminum that may originate from elastomeric components or processing aids.
Together, these methods provide a complete analytical profile of extractables and leachables in ophthalmic systems.
Compare GC-MS vs LC-MS in Extractables and Leachables Testing.
Container Closure Design and Mandatory Stability Evaluations
Ophthalmic packaging systems must balance sterility assurance, dosing accuracy, and mechanical usability. Regulatory compliance requires evaluation of physical performance alongside chemical safety.
Ophthalmic Stability and Structural Attributes
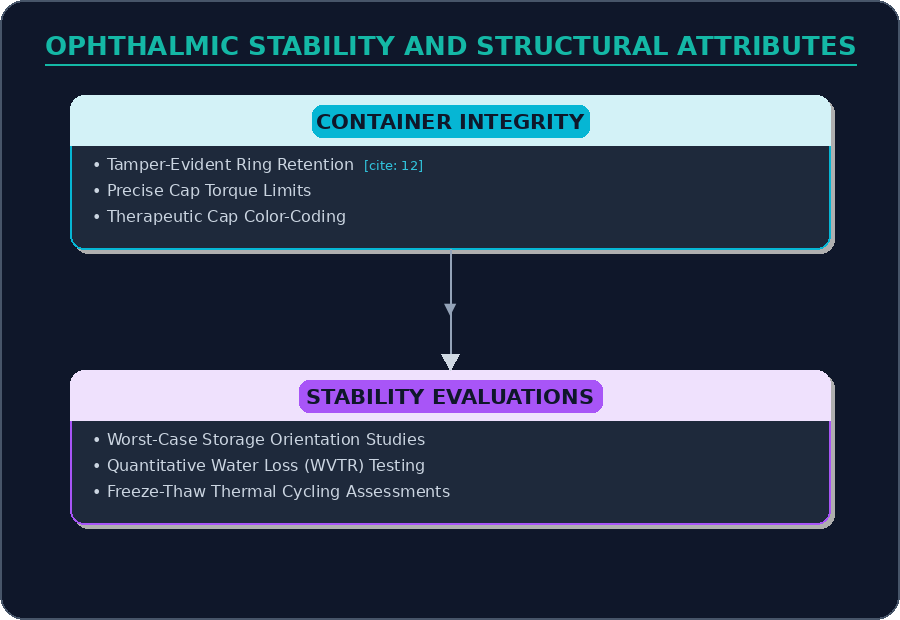
The mechanical design of ophthalmic bottles must balance ease of use with secure closure integrity. Opening force should be low enough for elderly patients while still maintaining sufficient seal strength to prevent leakage during transport.
Multi-dose containers require tamper-evident features that remain attached after first opening to prevent accidental contamination. For single-dose preservative-free systems, FDA guidance recommends a maximum fill volume of 0.5 mL to reduce reuse risk and microbial exposure.
Stability Evaluation Requirements
Storage Orientation: Stability studies must include upright and inverted orientations. Inversion ensures continuous contact between formulation and closure components, allowing realistic evaluation of leachable migration and potential leakage pathways.
Water Loss Testing (WVTR): Because LDPE is semipermeable, water vapor transmission testing is required to quantify moisture loss over time. This ensures container systems maintain product stability under low-humidity conditions.
Freeze-Thaw Cycling: Products such as emulsions, suspensions, and gels must undergo repeated freeze-thaw cycles, typically three cycles, to assess physical stability, phase separation, particle size changes, and redispersibility after temperature stress.
Strategic Conclusions on Extractables & Leachables Testing for Ophthalmic Drug Products
Mitigating chemical migration risks in topical ophthalmic formulations requires a clear understanding of polymer semipermeability, formulation thermodynamics, and the contribution of secondary packaging contaminants. Engaging a specialized testing provider to perform Extractables & Leachables Testing for Ophthalmic Drug Products is a critical step toward achieving global regulatory compliance and ensuring patient safety.
The high semipermeability of LDPE means that secondary packaging components, including inks, adhesives, and carton materials, frequently become the primary sources of chemical migration. As a result, a comprehensive extractables and leachables program must assess both primary container resins and secondary packaging systems. This evaluation depends on highly sensitive, validated analytical workflows using GC-MS/MS, LC-MS/MS, and ICP-MS to ensure that both organic and inorganic impurities are consistently monitored below the mandatory 1 ppm reporting threshold.
Read about specific EL Testing for Pre-filled Syringes.
For pharmaceutical developers, implementing a validated testing strategy is essential to support high-quality regulatory submissions and streamline approval timelines. ResolveMass Laboratories Inc. supports these requirements by providing advanced analytical services specifically designed for ophthalmic and parenteral drug products. Through rigorous simulation modeling and orthogonal screening approaches, ResolveMass Laboratories Inc. assists developers in addressing the complexities of container closure system evaluation.
To discuss your testing program and explore regulatory support options, contact our scientific team at:
https://resolvemass.ca/contact/
Frequently Asked Questions
The FDA uses concentration-based limits such as 1 ppm for reporting, 10 ppm for identification, and 20 ppm for qualification because ophthalmic drugs act directly on sensitive eye tissues. Even very small amounts of a leachable can create high local exposure in the ocular environment. This increases the risk of irritation, corneal damage, or sensitization. Systemic daily intake limits do not reflect these localized effects, which is why concentration-based controls are more appropriate.
LDPE has a semipermeable structure that allows small organic molecules to pass through it over time. Volatile compounds from inks, adhesives, labels, and varnishes first accumulate in the surrounding air space inside the packaging. From there, they dissolve into the outer surface of the container. These molecules then slowly diffuse through the polymer wall and enter the liquid formulation inside.
The Analytical Evaluation Threshold (AET) is derived from the Safety Concern Threshold (SCT) by adjusting it according to the product’s dosing volume and usage pattern. A simplified expression is AET estimated = SCT divided by Maximum Daily Dose (MDD). This gives a concentration-based limit for detection. The final AET is then refined using an uncertainty factor to account for variability in analytical response and ensure reliable detection of unknown compounds.
Water-only extraction does not fully represent real ophthalmic formulations because most products contain surfactants, preservatives, or viscosity enhancers. These ingredients can significantly change how chemical additives are extracted from packaging materials. They may enhance or accelerate leaching of hydrophobic compounds. Therefore, mixed solvent systems or formulation-mimicking media are required for realistic extractables and leachables assessment.
Benzalkonium chloride (BKC) can bind to hydrophobic surfaces like plastic containers over time. This reduces the amount of preservative remaining in the solution. If the concentration drops too much, the antimicrobial protection may become insufficient. This increases the risk of microbial contamination and can compromise both product safety and shelf-life performance.
Ophthalmic caps must strike a balance between usability and secure sealing. The opening force should be low enough for elderly or patients with limited hand strength to use comfortably. At the same time, the closure must maintain strong container integrity during transport and storage. Multi-dose systems also require a tamper-evident ring that stays attached after first opening to prevent accidental contamination.
Stability studies use different storage positions to ensure all container parts interact with the formulation. Inverted or horizontal storage keeps the liquid in continuous contact with the cap, tip, and sealing surfaces. This helps evaluate potential leachables from these components under worst-case conditions. It also helps detect leakage risks that might not appear in upright storage.
Reference:
- Guan, H., Han, X., Sun, J., Wang, J., Ning, B., Sun, H., & Zhao, X. (2025). Study on the adsorption behavior of preservatives in multidose eye drops and their interaction with packaging materials. ACS Omega, 10(49), 60733–60743. https://doi.org/10.1021/acsomega.5c08314
- Kuzmič, S., Zlobec, T., Sollner Dolenc, M., Roškar, R., & Trdan Lušin, T. (2026). Extractables and leachables in pharmaceutical products: Potential adverse effects and toxicological risk assessment. Toxics, 14(1), 92. https://doi.org/10.3390/toxics14010092
- United States Pharmacopeia. (n.d.). Extractables and leachables. https://www.usp.org/impurities/extractables-and-leachables
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. (2025, September). ICH Q3E: Guideline for extractables and leachables: Step 2 draft guideline – Released for comments [PowerPoint slides]. https://database.ich.org/sites/default/files/ICH_Q3E_Step2_Presentation_2025_0826.pdf
- Joseph, J. L. J., Rathore, S. S., Manjula, D., & Barnabas, W. (2025). Packaging, container, and closure of ophthalmic products. In N. K. Mehra (Ed.), Complex ophthalmic dosage forms: Advances in biomedical applications and future perspectives (pp. 355–392). Springer Nature Singapore. https://doi.org/10.1007/978-981-96-6306-4_12
- Momokawa, Y., Iida, M., Asada, H., & Fujisawa, T. (2023). Silver-salt-containing ophthalmic aqueous composition with which resin container is filled (European Patent Application No. EP4129341A1). European Patent Office. https://patents.google.com/patent/EP4129341A1/en

